
Anatomical Variations and Anomalies — MCQs

On this page
Which of the following are congenital abnormalities of the gall bladder? I. The phrygian cap II. Floating gall bladder III. Absence of gall bladder IV. Spigelian gall bladder Select the correct answer using the code given below :
The most common site of urethral opening in cases of hypospadias is :
Dysphagia lusoria is a condition which results from
All of the following are congenital sinuses except:
Which of the following are probable sites for Ectopic pancreas? 1. Submucosa of the stomach and duodenum 2. Liver 3. Small bowel mesentery 4. Splenic hilum
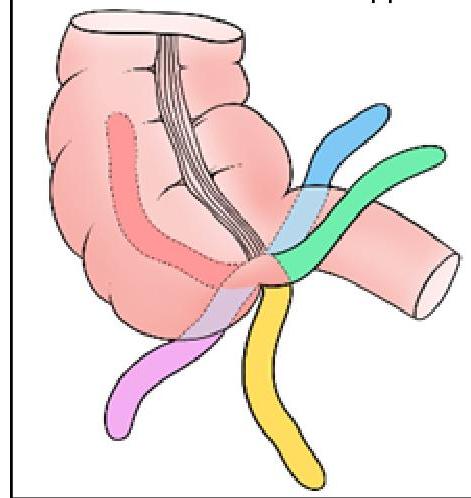
Identify the position of the appendix marked in BLACK in the given image:
In pediatric assessment, a cephalic index of 75-80 is classified as:
A skull is classified as dolichocephalic when the cephalic index is
Yoyo reflex is seen in:
Which of the following is an atavistic epiphysis?
Practice by Chapter
Principles of Anatomical Variations
Practice Questions
Variations in Vascular Anatomy
Practice Questions
Variations in Musculoskeletal System
Practice Questions
Variations in Nervous System
Practice Questions
Variations in Visceral Anatomy
Practice Questions
Clinically Significant Anatomical Variations
Practice Questions
Congenital Malformations
Practice Questions
Genetic Basis of Anatomical Variations
Practice Questions
Surgical Implications of Variations
Practice Questions
Imaging Aspects of Anatomical Variations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app