
Anatomical Variations and Anomalies — MCQs

On this page
The accessory obturator artery most commonly arises from which of the following arteries?
Where is the fabella typically present?
Which of the following statements about anodontia is false?
Dysphagia lusoria means dysphagia:
What is the term for a tongue anomaly?
A dens in dente is usually caused by:
Which of the following is the most common renal vascular anomaly?
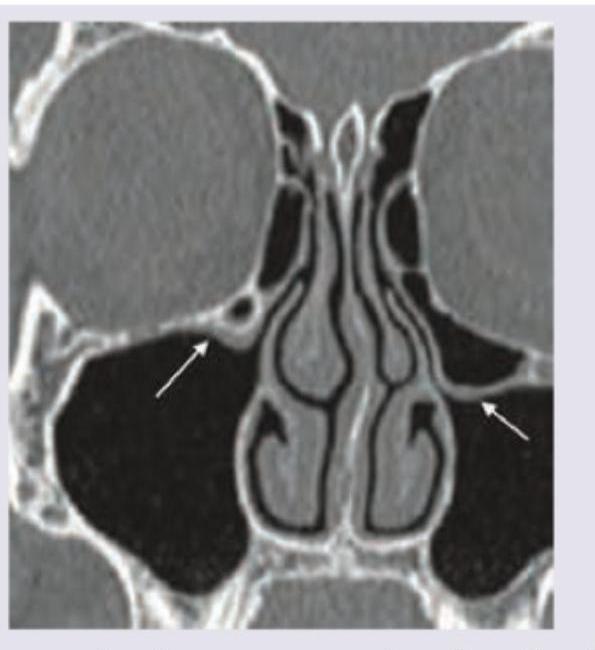
The CT scan of paranasal sinuses shows:
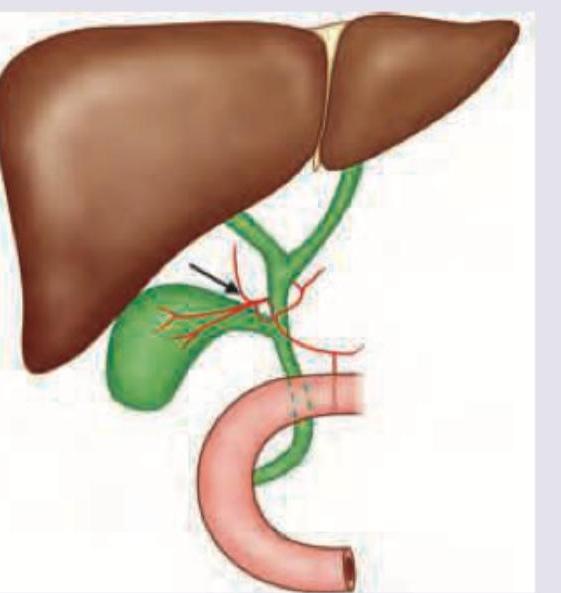
The following arrow marked vessel can cause torrential hemorrhage during cholecystectomy. Which of the following is the correct description?
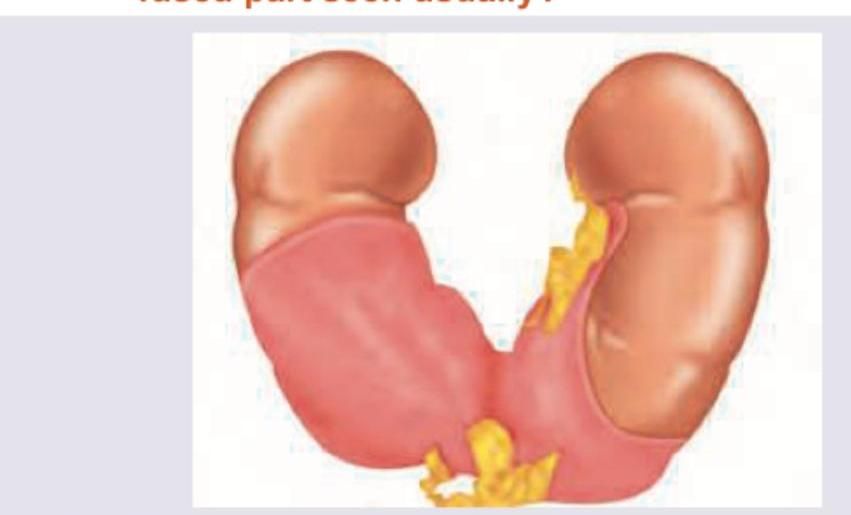
A 28 -year-old male was found to have a condition shown in the image below. At which level is the fused part seen usually?
Practice by Chapter
Principles of Anatomical Variations
Practice Questions
Variations in Vascular Anatomy
Practice Questions
Variations in Musculoskeletal System
Practice Questions
Variations in Nervous System
Practice Questions
Variations in Visceral Anatomy
Practice Questions
Clinically Significant Anatomical Variations
Practice Questions
Congenital Malformations
Practice Questions
Genetic Basis of Anatomical Variations
Practice Questions
Surgical Implications of Variations
Practice Questions
Imaging Aspects of Anatomical Variations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app