UPSC-CMS 2022 — Pathology
6 Previous Year Questions with Answers & Explanations
Which of the following statements regarding papillary thyroid cancer is correct? 1. It is the most common malignant tumour of thyroid gland. 2. It is more common in young females. 3. It has propensity for haematogenous spread. 4. Distant metastases are uncommon.
The maximum tensile strength that a wound can reach after healing is complete, in comparison to normal skin, is
Which one of the following is correct regarding Gastrointestinal Stromal Tumour (GIST)?
The commonest variety of peritoneal metastasis is
Which of the following are correct about glomus tumour? 1. It arises from Suquet-Hoyer canals. 2. Its usual site is nail bed. 3. It is usually a small purple nodule. 4. It is painless.
The following table shows some of the pneumoconioses diseases along with the most implicated causative chemical agents. Which among the following represent the correct combinations of diseases and causative chemical agents? Select the correct answer using the code given below.
UPSC-CMS 2022 - Pathology UPSC-CMS Practice Questions and MCQs
Question 1: Which of the following statements regarding papillary thyroid cancer is correct? 1. It is the most common malignant tumour of thyroid gland. 2. It is more common in young females. 3. It has propensity for haematogenous spread. 4. Distant metastases are uncommon.
- A. 2. It is more common in young females.
- B. 4. Distant metastases are uncommon.
- C. 3. It has propensity for haematogenous spread.
- D. 1. It is the most common malignant tumour of thyroid gland. (Correct Answer)
Explanation: ***1. It is the most common malignant tumour of thyroid gland.*** - **Papillary thyroid cancer (PTC)** accounts for approximately **80-85% of all thyroid cancers**, making it the most prevalent type [1]. - This is the definitive correct statement among the options provided. *2. It is more common in young females.* - While PTC is indeed **more common in females** (3:1 female-to-male ratio), the term "young" is imprecise for exam purposes [3]. - PTC typically occurs in the **3rd to 5th decades** (30-50 years), which is more accurately described as "middle-aged" rather than "young" [1], [2]. - The statement lacks specificity needed for a definitive answer. *3. It has propensity for haematogenous spread.* - This is **incorrect**. PTC primarily spreads via the **lymphatic system** to regional cervical lymph nodes [2]. - **Hematogenous spread** is characteristic of **follicular thyroid carcinoma**, not papillary type [2]. - While distant hematogenous metastases can occur in advanced PTC, it is **not** the characteristic pattern of spread. *4. Distant metastases are uncommon.* - While this statement has merit (distant metastases occur in only 5-10% at presentation), it is less definitively correct than statement 1. - The majority of PTC metastases are **locoregional lymphatic** spread rather than distant. - However, when distant metastases do occur, it affects prognosis significantly (lungs > bones). **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1098-1100. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 428-430. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1095-1096.
Question 2: The maximum tensile strength that a wound can reach after healing is complete, in comparison to normal skin, is
- A. 60%–80% (Correct Answer)
- B. 30%–50%
- C. 20%–30%
- D. 50%–60%
Explanation: ***60%–80%*** - A fully healed wound, after complete maturation (typically **3 months**), achieves approximately **70–80%** of the **tensile strength** of normal unwounded skin [1]. - This is the **maximum tensile strength** that can be attained despite ongoing **collagen remodeling** and cross-linking [1]. - The strength never reaches 100% because scar tissue has a different collagen architecture compared to normal tissue, with **Type I collagen** replacing the original dermis but in a less organized pattern. *50%–60%* - This range underestimates the final tensile strength achieved by completely healed wounds. - At approximately **6 weeks**, wounds may be at this strength level, but further maturation increases strength to 70–80% [1]. *20%–30%* - This represents the tensile strength at an **early stage** of wound healing (around 3 weeks). - By the time healing is **complete**, the tensile strength is substantially higher than this range. *30%–50%* - This range also underestimates the maximum tensile strength of fully healed wounds. - While this may represent intermediate stages of healing, the final mature scar achieves greater strength approaching 70–80%. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Inflammation and Repair, pp. 119-121.
Question 3: Which one of the following is correct regarding Gastrointestinal Stromal Tumour (GIST)?
- A. The male to female ratio is 9 : 1.
- B. 50% arise from stomach. (Correct Answer)
- C. Lymphatic spread is seen commonly.
- D. It arises from epithelial layer.
Explanation: ***50% arise from stomach.*** - The stomach is the most common primary site for GISTs, accounting for approximately **50-60% of cases**. [1] - Other common sites include the small intestine (25-30%), colon/rectum (5%), and esophagus (<5%). *The male to female ratio is 9 : 1.* - GISTs show **no significant gender predominance**, with the male-to-female ratio being roughly 1:1. - While some gastrointestinal cancers have gender disparities, GISTs affect both sexes almost equally. *Lymphatic spread is seen commonly.* - GISTs rarely spread via the **lymphatic system**; lymphatic metastases are uncommon. - The primary routes of GIST metastasis are **hematogenous** spread, commonly to the liver, and direct seeding within the peritoneal cavity. *It arises from epithelial layer.* - GISTs are **mesenchymal tumors**, specifically believed to originate from the **interstitial cells of Cajal** or their precursor cells. [1] - These cells are found in the muscularis propria layer of the gastrointestinal tract, not the epithelial layer. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Gastrointestinal Tract, pp. 782-784.
Question 4: The commonest variety of peritoneal metastasis is
- A. plaques of varying sizes
- B. drop metastasis in pelvis
- C. diffuse adhesion
- D. discrete nodules (Correct Answer)
Explanation: ***discrete nodules*** - Peritoneal metastasis most commonly manifests as **discrete nodules** scattered across the peritoneal surfaces [1]. - These nodules vary in size and distribution, often arising from the implantation of malignant cells shed from a primary tumor. *plaques of varying sizes* - While plaques can occur, they are generally less common than discrete nodules as the primary manifestation of **peritoneal carcinomatosis**. - Plaques often represent confluent growth of numerous smaller nodules rather than the initial, more frequent presentation. *drop metastasis in pelvis* - **Drop metastases** to the pelvis are a common site for peritoneal dissemination due to gravity and fluid dynamics within the peritoneal cavity. - However, referring to it as simply "drop metastasis in pelvis" describes a location rather than the morphology, which is typically **nodular**. *diffuse adhesion* - **Diffuse adhesions** typically result from chronic inflammation or surgical procedures, connecting peritoneal surfaces. - While extensive tumor growth can lead to adhesions, the initial and most common pattern of metastasis is individual **tumor cell implantation** forming **discrete nodules**, not diffuse initial adherence. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 233-234.
Question 5: Which of the following are correct about glomus tumour? 1. It arises from Suquet-Hoyer canals. 2. Its usual site is nail bed. 3. It is usually a small purple nodule. 4. It is painless.
- A. 1, 2 and 4
- B. 2, 3 and 4
- C. 1, 3 and 4
- D. 1, 2 and 3 (Correct Answer)
Explanation: ***1, 2 and 3*** - Glomus tumors originate from the **Suquet-Hoyer canals**, specialized arteriovenous anastomoses involved in thermoregulation. - They are most frequently found in the **nail bed** (especially subungual region) as small, **purple** (reddish-blue) nodules and are typically very painful. - The classic triad includes severe pain, cold sensitivity, and point tenderness. *1, 2 and 4* - This option incorrectly states that glomus tumors are **painless**. In fact, they are characterized by severe pain due to their rich innervation. - While correct that they arise from Suquet-Hoyer canals and are found in the nail bed, the **painlessness** aspect is inaccurate. *2, 3 and 4* - This option incorrectly includes the statement that glomus tumors are **painless**, which contradicts a key distinguishing feature. - Although glomus tumors are typically found in the nail bed and appear as purple nodules, pain is a characteristic clinical feature, not absence of pain. *1, 3 and 4* - This option incorrectly states that glomus tumors are **painless** and omits the correct statement about the usual nail bed location. - While they do arise from Suquet-Hoyer canals and can be small purple nodules, their characteristic severe pain makes this option incorrect.
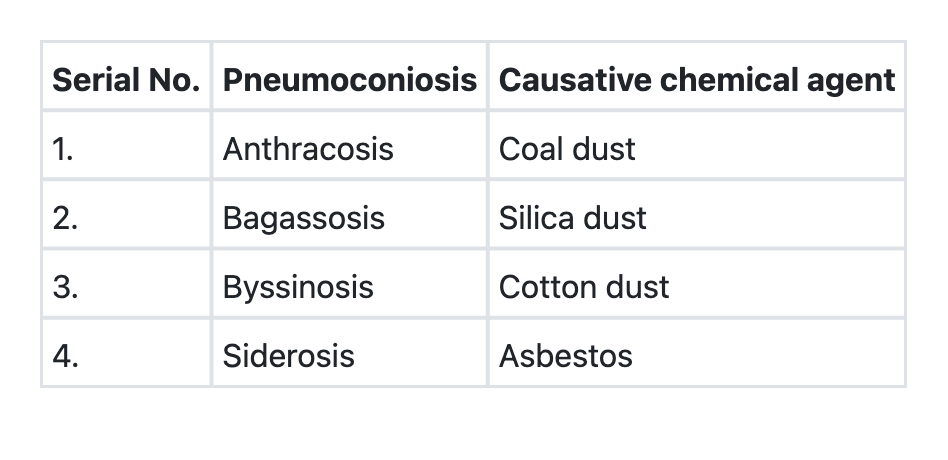
Question 6: The following table shows some of the pneumoconioses diseases along with the most implicated causative chemical agents. Which among the following represent the correct combinations of diseases and causative chemical agents? Select the correct answer using the code given below.
- A. 2 and 4
- B. 2 and 3
- C. 1 and 3
- D. 1 and 2 (Correct Answer)
Explanation: ***Correct: 1 and 2*** - **Statement 1 (Anthracosis - Coal dust)** is correct. Anthracosis, also known as **coal worker's pneumoconiosis**, is caused by chronic inhalation of coal dust particles [1]. - **Statement 2 (Byssinosis - Cotton dust)** is correct. Byssinosis is an occupational lung disease affecting **textile workers** exposed to cotton, flax, or hemp dust, causing airway obstruction. *Incorrect: 2 and 4* - Statement 4 is incorrect. **Siderosis** is caused by inhalation of **iron dust** (common in welders and miners), not asbestos [1]. Asbestos exposure causes **asbestosis** [1]. *Incorrect: 2 and 3* - Statement 3 is incorrect. **Bagassosis** is caused by inhalation of **sugarcane bagasse dust** (a hypersensitivity pneumonitis), not silica dust [1]. Silica causes **silicosis** [1]. *Incorrect: 1 and 3* - While statement 1 is correct (Anthracosis - Coal dust), statement 3 is incorrect as explained above (Bagassosis is caused by sugarcane bagasse dust, not silica dust) [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, p. 695.