All (119)Anatomy (3)Anesthesiology (1)Biochemistry (1)Community Medicine (34)Dermatology (1)Forensic Medicine (2)Internal Medicine (10)Microbiology (3)Obstetrics and Gynecology (32)Orthopaedics (4)Pathology (2)Pharmacology (3)Radiology (2)Surgery (21)
Q91
Pentavalent vaccine provides protection against which of the following diseases?
Q92
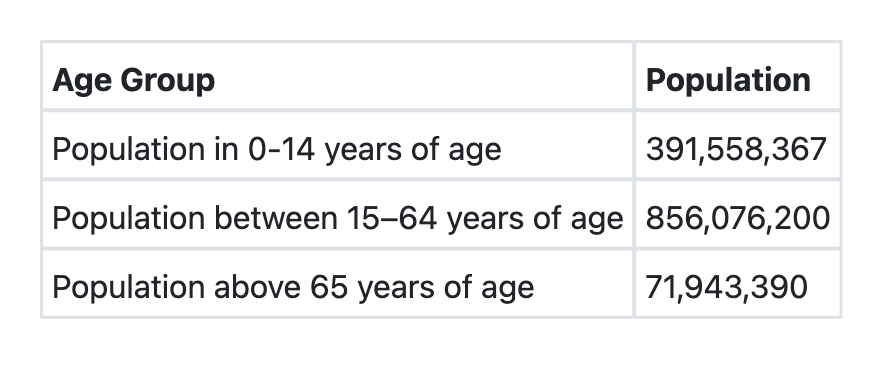
Consider the following data for a country: What shall be the dependency ratio of this country?
Q93
Which one of the following statements regarding Rabies Immunoglobulin is NOT true?
Q94
Visual inspection based screening test with 5 % acetic acid is used for the screening of which one of the following cancers?
Q95
Predictive accuracy of a screening test depends on the following EXCEPT:
Q96
How much of Zinc supplement is recommended by WHO and UNICEF for infants less than 6 months of age after an episode of acute diarrhoea?
Q97
Which one of the following statements regarding sequential administration of Inactivated Polio Vaccine (IPV) and Oral Polio Vaccine (OPV) is NOT correct?