Q11
Which one of the following is NOT a contagious disease?
Q12
Pentavalent vaccine provides protection against which of the following diseases?
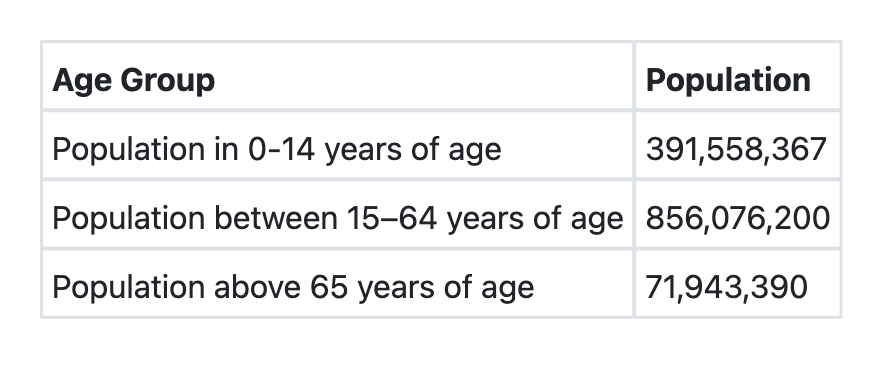
Q13
Consider the following data for a country: What shall be the dependency ratio of this country?
Q14
Which one of the following statements regarding Rabies Immunoglobulin is NOT true?
Q15
Visual inspection based screening test with 5 % acetic acid is used for the screening of which one of the following cancers?
Q16
Predictive accuracy of a screening test depends on the following EXCEPT:
Q17
How much of Zinc supplement is recommended by WHO and UNICEF for infants less than 6 months of age after an episode of acute diarrhoea?
Q18
Which one of the following statements regarding sequential administration of Inactivated Polio Vaccine (IPV) and Oral Polio Vaccine (OPV) is NOT correct?
Q19
All of the following are global targets for WHO Global Action Plan (2013–2020) for Prevention and Control of NCDs, EXCEPT:
Q20
Under the Employees State Insurance (ESI) Scheme, extended sickness benefit is provided in which of the following infectious diseases? 1. Tuberculosis 2. Leprosy 3. Chronic empyema Select the correct answer using the code given below: