All (119)Anatomy (5)Biochemistry (1)Community Medicine (35)ENT (2)Forensic Medicine (1)Internal Medicine (5)Obstetrics and Gynecology (31)Orthopaedics (1)Pathology (2)Pediatrics (5)Pharmacology (2)Physiology (2)Radiology (1)Surgery (26)
Q11
Asymptomatic carriers of pathogenic organisms are called:
Q12
A cohort study was conducted among 200 men aged 20–30 years in Rampur village. Out of 200, 120 men were tobacco users and rest 80 didn’t take any form of tobacco. At the end of one year, 40 men among tobacco users and 10 men among non-tobacco users developed tuberculosis. The incidence of tuberculosis among tobacco users is:
Q13
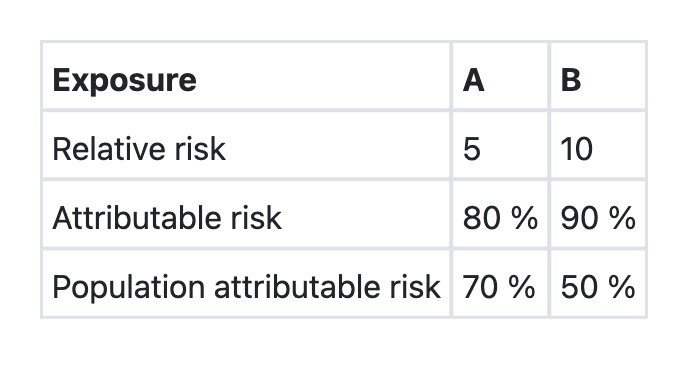
The data regarding two exposures A and B, associated with a disease X in a community is given below: Which one of the following assertions and the reasons given is correct?
Q14
Which of the following types of study designs will be most appropriate to find out the association between mobile phone radiation exposure and cancer?
Q15
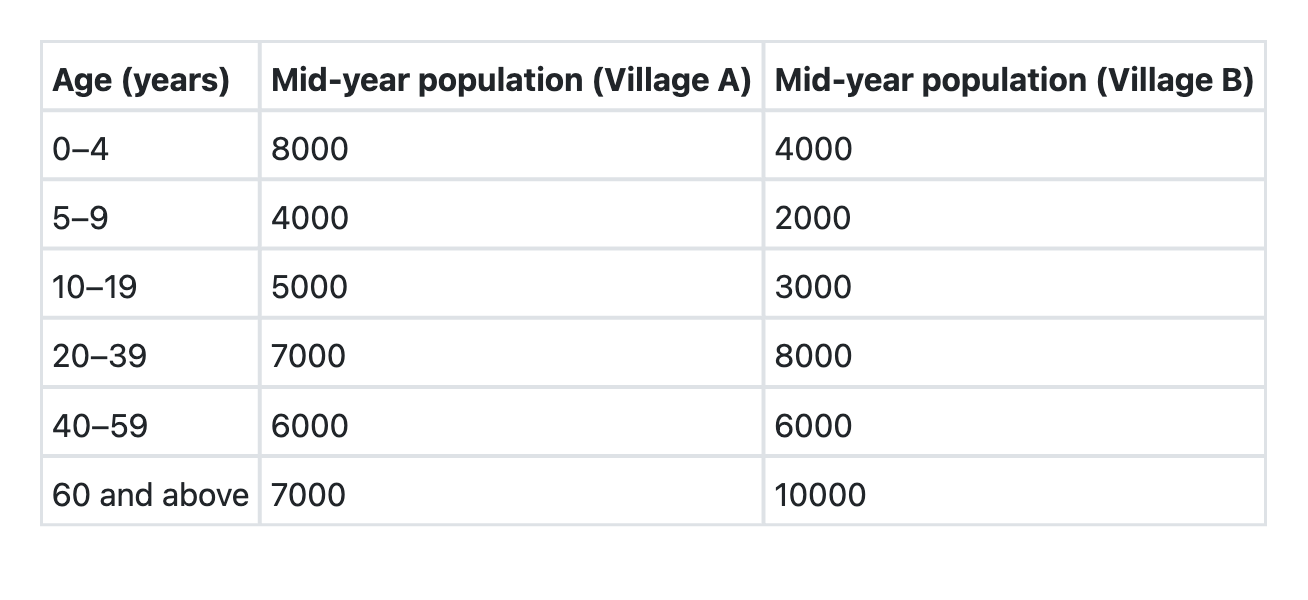
The villages A and B have the following age compositions: Which of the following is the best indicator for comparing the death rates of these two villages?
Q16
Which of the following is/are suggested by rising incidence rates of any disease? 1. Need for a new disease control programme 2. Improvement in reporting practices 3. Change in the etiology of the disease Select the correct answer using the codes given below:
Q17
What constitutes the denominator in ‘Total Dependency Ratio’?