All (115)Anatomy (4)Biochemistry (1)Community Medicine (36)Dermatology (2)General Medicine (1)Internal Medicine (3)Microbiology (2)Obstetrics and Gynecology (26)Ophthalmology (2)Pathology (4)Pediatrics (2)Pharmacology (3)Physiology (1)Surgery (28)
Q61
Medical management of tubal ectopic pregnancy can be done in the following EXCEPT:
Q62
Which of the following genital infections is associated with preterm labour?
Q63
Multiple pregnancy is associated with an increased incidence of the following EXCEPT:
Q64
Surgical staging is done for all the genital malignancies EXCEPT:
Q65
B-Lynch suture for atonic postpartum haemorrhage:
Q66
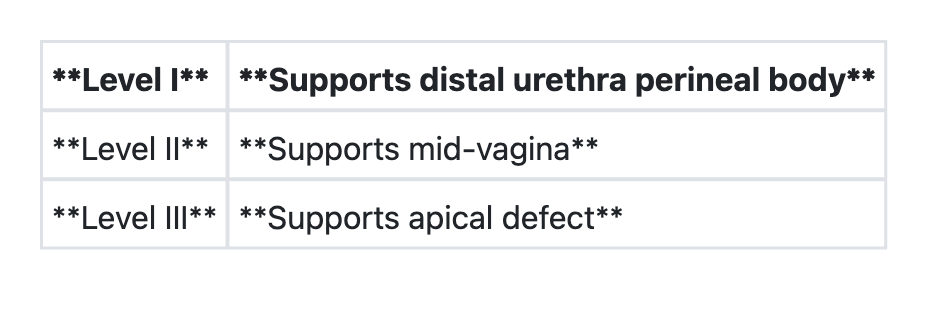
Regarding 'DeLancey's levels of vaginal support', consider the following pairs:
Q67
Consider the following pairs regarding foetal heart during labour:
