Q11
Where are antisperm antibodies usually present?
Q12
Modified Bishop’s score includes all EXCEPT:
Q13
The engaging diameter of brow presentation is:
Q14
Which of the following is/are the risk factors for acute pelvic inflammatory disease in women? 1. Intercourse during menstruation 2. Multiple sex partners Select the correct answer using the code given below:
Q15
Medical management of tubal ectopic pregnancy can be done in the following EXCEPT:
Q16
Which of the following genital infections is associated with preterm labour?
Q17
Multiple pregnancy is associated with an increased incidence of the following EXCEPT:
Q18
Surgical staging is done for all the genital malignancies EXCEPT:
Q19
B-Lynch suture for atonic postpartum haemorrhage:
Q20
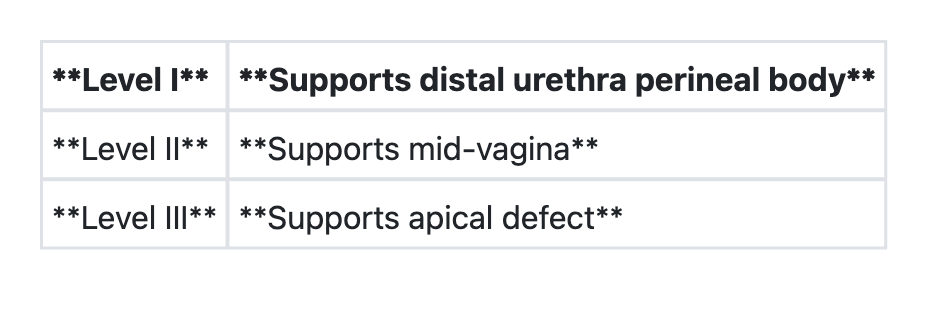
Regarding 'DeLancey's levels of vaginal support', consider the following pairs: