Districts are classified into different categories regarding neonatal tetanus risk. Which one of the following correctly describes 'Neonatal Tetanus Elimination' status?
Influenza vaccine is recommended for: 1. Elderly 2. Persons with underlying chronic diseases 3. HIV infected 4. General population Select the correct answer using the code given below:
Consider the following features of food poisoning: 'Incubation period less than 24 hours, source of infection is milk products, and symptoms include diarrhoea and vomiting.' To which of the following does the above description apply? 1. Staphylococcal food poisoning 2. Salmonella food poisoning 3. Botulism Select the correct answer using the code given below:
For adolescents, what is the weekly iron and folic acid supplementation dose?
Which of the following statements is/are true about proportional case rate of malaria? 1. This indicator is used since morbidity rate is difficult to determine 2. This is defined as the number of cases of malaria for every 100 patients seen in hospital OPDs 3. It is a crude index since cases are not related to their time and space distribution Select the correct answer using the code given below:
Consider the following statements: 1. Type 2 poliovirus was eliminated in India in 2005. 2. Main cause of vaccine derived polioviruses (VDPV) is Type 2 component of OPV. Which of the statements given above is/are correct?
Which of the following statements is true about hydatid disease?
Which of the following statements is true about direct age standardization?
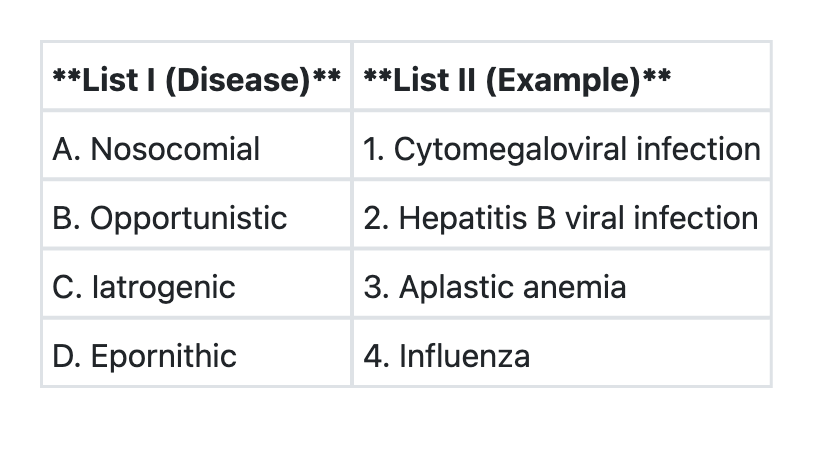
Match List I with List II and select the correct answer using the codes given below the lists:
With reference to International Certificate of Vaccination for Yellow Fever, the validity of the certificate begins how many days after the vaccination?
UPSC-CMS 2016 - Community Medicine UPSC-CMS Practice Questions and MCQs
Question 21: Districts are classified into different categories regarding neonatal tetanus risk. Which one of the following correctly describes 'Neonatal Tetanus Elimination' status?
- A. Incidence rate between 1 to 2/1000 births, three doses of TT vaccine coverage 70%, attended deliveries more than 75%
- B. Incidence rate 0.5 to 1/1000 births, three doses of TT vaccine coverage between 70% and 80%, attended deliveries between 65% and 70%
- C. Incidence rate more than 2/1000 births, two doses of TT vaccine coverage less than 70%, attended deliveries between 60% and 70%
- D. Incidence rate less than 0.1/1000 births, two doses of TT vaccine coverage more than 90%, attended deliveries more than 75% (Correct Answer)
Explanation: ***Incidence rate less than 0.1/1000 births, two doses of TT vaccine coverage more than 90%, attended deliveries more than 75%*** - **Neonatal Tetanus Elimination (NTE)** is defined by the World Health Organization (WHO) as achieving **less than 1 case of neonatal tetanus per 1,000 live births** in every district of a country. - India has set more stringent operational criteria for district classification, with **high performance districts** achieving rates below 0.1 per 1,000 live births. - Elimination status is achieved through **high tetanus toxoid (TT) vaccination coverage** in pregnant women (>90% with at least two doses) and a **high proportion of institutional/attended deliveries** (>75%) by skilled birth attendants. - These combined interventions ensure that most newborns are protected through maternal antibodies and delivered in hygienic conditions. *Incidence rate between 1 to 2/1000 births, three doses of TT vaccine coverage 70%, attended deliveries more than 75%* - An incidence rate of 1 to 2 cases per 1,000 live births indicates **failure to achieve elimination status**, as it exceeds the WHO threshold of <1 per 1,000 live births. - **TT vaccine coverage of only 70%** is insufficient for elimination; the program requires >90% coverage to generate herd immunity and maternal protection. - While attended deliveries >75% is adequate, the combination of high incidence and low vaccine coverage indicates this district is still at risk. *Incidence rate 0.5 to 1/1000 births, three doses of TT vaccine coverage between 70% and 80%, attended deliveries between 65% and 70%* - An incidence rate between 0.5 and 1 per 1,000 live births is **borderline but still above the elimination threshold**. - **TT vaccine coverage of 70-80%** and **attended delivery rates of 65-70%** are suboptimal and need significant improvement. - This represents a moderate-risk district that requires intensified efforts in both immunization and safe delivery practices. *Incidence rate more than 2/1000 births, two doses of TT vaccine coverage less than 70%, attended deliveries between 60% and 70%* - An incidence rate exceeding 2 cases per 1,000 live births clearly indicates a **high-risk district**, far from achieving elimination. - **Low TT vaccine coverage (<70%)** leaves a large proportion of pregnant women and their newborns unprotected. - **Suboptimal attended delivery rates (60-70%)** mean many births occur in unhygienic conditions, increasing tetanus risk through umbilical stump contamination.
Question 22: Influenza vaccine is recommended for: 1. Elderly 2. Persons with underlying chronic diseases 3. HIV infected 4. General population Select the correct answer using the code given below:
- A. 2 and 3 only
- B. 4
- C. 1 and 2 only
- D. 1, 2 and 3 (Correct Answer)
Explanation: ***1, 2 and 3*** - **Influenza vaccine** is broadly recommended for individuals at higher risk of complications, which explicitly includes the **elderly**, persons with **underlying chronic diseases**, and the **HIV-infected**. - These groups often experience more severe illness, hospitalizations, and mortality from influenza infection. *2 and 3 only* - This option correctly identifies **persons with underlying chronic diseases** and the **HIV-infected** as recommendation groups. - However, it incorrectly excludes the **elderly**, who are a primary target group for influenza vaccination due to age-related immune senescence. *4* - While influenza vaccination is increasingly encouraged for the general population due to community benefits, the question asks for groups where it is specifically recommended for individual protection, focusing on those at higher risk. - This option is too broad and doesn't highlight the specific at-risk groups mentioned. *1 and 2 only* - This option correctly includes the **elderly** and **persons with underlying chronic diseases**. - However, it incorrectly omits the **HIV-infected**, who are also a priority group for influenza vaccination due to their immunocompromised status.
Question 23: Consider the following features of food poisoning: 'Incubation period less than 24 hours, source of infection is milk products, and symptoms include diarrhoea and vomiting.' To which of the following does the above description apply? 1. Staphylococcal food poisoning 2. Salmonella food poisoning 3. Botulism Select the correct answer using the code given below:
- A. 1 only (Correct Answer)
- B. 2 only
- C. 1 and 3
- D. 1 and 2
Explanation: ***1 only*** - **Staphylococcal food poisoning** has a **very short incubation period** (1-6 hours), making it the most characteristic match for "less than 24 hours." - Commonly associated with contaminated **dairy products** (milk, cream, custards) and meats where the bacteria produce **preformed enterotoxins**. - Causes **sudden onset** of severe **nausea, vomiting**, and diarrhea due to preformed toxins. - The **rapid onset** (within hours) and strong association with **milk products** make this the best fit for all three criteria. *2 only* - **Salmonella food poisoning** typically has an incubation period of **6-72 hours** (average 12-36 hours), which is longer than the typical Staphylococcal onset. - While technically some cases can present within 24 hours, the **short incubation period** described is more characteristic of **toxin-mediated** rather than **infection-mediated** food poisoning. - Primary sources are **poultry, eggs**, and meat; while milk can be a vehicle, it's not the classic source. - Symptoms result from **bacterial invasion** of intestinal mucosa rather than preformed toxins. *1 and 3* - While **Staphylococcal food poisoning** aligns with the description, **Botulism** does not. - **Botulism** has an incubation period of **12-36 hours** (range 2 hours to 8 days) and is characterized by **neurological symptoms** (diplopia, dysphagia, descending paralysis) rather than prominent diarrhea and vomiting. - Source is typically **improperly canned or preserved foods**, not milk products. *1 and 2* - **Salmonella food poisoning** has a longer average incubation period and is more commonly associated with poultry and eggs, differentiating it from the described scenario. - The **very short incubation period** (< 24 hours, typically 1-6 hours) and **milk products** as source point specifically to **Staphylococcal food poisoning** with its preformed toxin mechanism. - Only **Staphylococcal food poisoning** matches all conditions most characteristically.
Question 24: For adolescents, what is the weekly iron and folic acid supplementation dose?
- A. 60 mg elemental iron and 400 microgram folic acid
- B. 120 mg elemental iron and 400 microgram folic acid
- C. 150 mg elemental iron and 500 microgram folic acid
- D. 100 mg elemental iron and 500 microgram folic acid (Correct Answer)
Explanation: ***100 mg elemental iron and 500 microgram folic acid*** - This is the **current recommended dosage** for India's **Weekly Iron and Folic Acid Supplementation (WIFS) program** for adolescents (10-19 years). - The **Government of India's National Health Mission** and **WHO guidelines** endorse this specific amount for weekly supplementation to prevent and control **iron deficiency anemia** in adolescents. - This dosage is used in school-based and community programs across India. *120 mg elemental iron and 400 microgram folic acid* - This was an **earlier recommendation** that has since been updated to the current standard of 100 mg + 500 mcg. - While previously used, current WIFS guidelines have standardized the dose at **100 mg elemental iron** and **500 mcg folic acid**. *60 mg elemental iron and 400 microgram folic acid* - **60 mg elemental iron** is typically a **daily therapeutic dose** or used for younger children, and is insufficient for weekly prophylactic supplementation in adolescents. - This lower dose would not provide adequate coverage for the weekly supplementation schedule. *150 mg elemental iron and 500 microgram folic acid* - This dose of **elemental iron (150 mg)** is higher than the standard weekly recommendation (100 mg) for routine adolescent supplementation. - The higher iron dose is not necessary for general prophylactic supplementation and could increase the risk of gastrointestinal side effects.
Question 25: Which of the following statements is/are true about proportional case rate of malaria? 1. This indicator is used since morbidity rate is difficult to determine 2. This is defined as the number of cases of malaria for every 100 patients seen in hospital OPDs 3. It is a crude index since cases are not related to their time and space distribution Select the correct answer using the code given below:
- A. 2 only
- B. 3 only
- C. 1, 2 and 3 (Correct Answer)
- D. 2 and 3 only
Explanation: ***1, 2 and 3*** - All three statements accurately describe the **proportional case rate of malaria** (also known as proportional morbidity). - Statement 1 is correct: This indicator is used because calculating true **morbidity rates** requires accurate population denominator data, which is often difficult to obtain in resource-limited settings. The proportional case rate provides a practical alternative using hospital-based data. - Statement 2 is correct: It is defined as **(Number of malaria cases / Total OPD patients) × 100**, representing malaria cases per 100 patients seen in hospital outpatient departments. - Statement 3 is correct: It is a **crude index** because it's a ratio (not a true rate) that doesn't account for the population at risk, temporal trends, or geographical distribution of cases. It merely reflects the relative burden among those seeking care. *2 only* - This option is incomplete. While statement 2 correctly defines the calculation method, it incorrectly excludes statements 1 and 3, which are also true. - The proportional case rate is indeed calculated as malaria cases per 100 OPD patients, but this alone doesn't explain its purpose or limitations. *3 only* - This option is incomplete. While statement 3 correctly identifies it as a **crude index** with limitations in temporal and spatial analysis, it incorrectly excludes statements 1 and 2. - Understanding why it's crude (statement 3) without knowing why it's used (statement 1) and how it's calculated (statement 2) provides an incomplete picture. *2 and 3 only* - This option is incomplete. While statements 2 and 3 are both correct, it incorrectly excludes statement 1. - The fundamental rationale for using proportional case rate—the difficulty in determining true morbidity rates—is missing, making this option less comprehensive than the correct answer.
Question 26: Consider the following statements: 1. Type 2 poliovirus was eliminated in India in 2005. 2. Main cause of vaccine derived polioviruses (VDPV) is Type 2 component of OPV. Which of the statements given above is/are correct?
- A. Both 1 and 2
- B. 1 only
- C. 2 only (Correct Answer)
- D. Neither 1 nor 2
Explanation: ***2 only*** - Statement 2 is **correct**: The **Type 2 component of OPV** is the primary cause of vaccine-derived polioviruses (VDPV) due to its higher propensity to revert to neurovirulent forms compared to Types 1 and 3. - This significant risk led to the **global withdrawal of Type 2 from OPV** in April 2016, when the world switched from trivalent OPV (tOPV) to bivalent OPV (bOPV containing only Types 1 and 3). - Statement 1 is **incorrect**: The last **wild Type 2 poliovirus case in India was detected in 1999** (Aligarh, UP), not 2005. WHO declared wild poliovirus Type 2 **globally eradicated in September 2015**. *Both 1 and 2* - This is incorrect because statement 1 contains a factual error about the timing of Type 2 poliovirus elimination in India (1999, not 2005). - Only statement 2 is correct. *1 only* - This is incorrect because statement 1 is **factually wrong** - Type 2 poliovirus was eliminated from India in **1999, not 2005**. - The last wild Type 2 case globally was also in India (1999), making this statement doubly incorrect. *Neither 1 nor 2* - This is incorrect because statement 2 is **completely accurate** - Type 2 component of OPV is indeed the main cause of VDPV. - The high rate of genetic reversion and neurovirulence of OPV Type 2 necessitated its removal from routine immunization schedules worldwide.
Question 27: Which of the following statements is true about hydatid disease?
- A. It is a protozoal disease
- B. It is a zoonosis (Correct Answer)
- C. Man is the definitive host
- D. It is rare in sheep rearing countries
Explanation: ***Correct: It is a zoonosis*** - Hydatid disease is caused by the larval stage of **Echinococcus granulosus**, a **tapeworm**, and is transmitted from animals to humans - **Zoonoses** are diseases that can be transmitted from animals to humans, making this the correct statement - The primary reservoir includes dogs (definitive hosts) and sheep (intermediate hosts), with transmission to humans occurring through contact with contaminated dog feces *Incorrect: It is a protozoal disease* - Hydatid disease is caused by a **tapeworm** (cestode), specifically *Echinococcus granulosus*, not by a protozoan - Protozoal diseases are caused by single-celled eukaryotic organisms such as *Plasmodium* (malaria) or *Giardia* (giardiasis) - This is a helminthic infection, not a protozoal one *Incorrect: Man is the definitive host* - In the life cycle of *Echinococcus granulosus*, **dogs and other canines** are the **definitive hosts**, harboring the adult tapeworm in their intestines - Humans are **accidental intermediate hosts**, getting infected by ingesting eggs and developing hydatid cysts in organs (especially liver and lungs) - The natural cycle involves dogs eating infected offal from sheep, not humans being part of the natural transmission cycle *Incorrect: It is rare in sheep rearing countries* - Hydatid disease is **endemic** and more common in **sheep-rearing countries** including Mediterranean regions, Middle East, South America, Australia, and parts of Africa - Sheep act as important intermediate hosts in the life cycle of *Echinococcus granulosus* - The dog-sheep-dog cycle maintains high endemicity in pastoral communities where dogs have access to infected sheep viscera
Question 28: Which of the following statements is true about direct age standardization?
- A. Number of people in each age group is not known
- B. Age specific death rates are not known
- C. A standard population is used (Correct Answer)
- D. Standardized mortality ratio is used
Explanation: ***A standard population is used*** - In **direct age standardization**, age-specific death rates from the study population are applied to a **standard population's** age distribution to calculate an expected number of events. - This method helps to compare mortality or morbidity across different populations by removing the confounding effect of differing age structures. *Number of people in each age group is not known* - This statement is incorrect; to apply the study population's age-specific rates to the standard population, the **number of people in each age group of the standard population must be known**. - Without this demographic information, direct age standardization cannot be performed effectively. *Age specific death rates are not known* - This statement is incorrect because **age-specific death rates** for the *study population* are a prerequisite for direct age standardization. - These rates are multiplied by the corresponding age groups of a **standard population** to calculate standardized rates. *Standardized mortality ratio is used* - The **Standardized Mortality Ratio (SMR)** is a measure used in *indirect* age standardization, not direct age standardization. - SMR compares the number of observed deaths in a study population to the number expected if the study population had the same age-specific death rates as a **standard population**.
Question 29: Match List I with List II and select the correct answer using the codes given below the lists:
- A. A->2 B->1 C->3 D->4
- B. A->1 B->2 C->4 D->3
- C. A->2 B->1 C->4 D->3 (Correct Answer)
- D. A->1 B->2 C->3 D->4
Explanation: ***A->2 B->1 C->4 D->3*** **Correct Matching:** **A. Nosocomial → Hepatitis B viral infection (2)** - **Nosocomial infections** are hospital-acquired infections contracted in healthcare settings - **Hepatitis B** can be transmitted nosocomially through contaminated needles, medical equipment, blood products, or during invasive procedures - This is a classic example of nosocomial transmission **B. Opportunistic → Cytomegaloviral infection (1)** - **Opportunistic infections** occur in individuals with compromised immune systems - **CMV infection** is a prototypical opportunistic pathogen, commonly affecting: - HIV/AIDS patients with CD4 count <50 - Solid organ transplant recipients - Bone marrow transplant patients - Patients on immunosuppressive therapy **C. Iatrogenic → Influenza (4)** - **Iatrogenic conditions** are inadvertently caused by medical treatment or procedures - This pairing is clinically weak as influenza is primarily a community-acquired respiratory infection, not caused by medical intervention - This represents the official answer key matching for this PYQ **D. Epornithic → Aplastic anemia (3)** - **Epornithic** refers to epidemic disease outbreaks in bird populations - This pairing is clinically incorrect as aplastic anemia is a human bone marrow failure disorder - This represents the official answer key matching for this PYQ **Note:** This is a Past Year Question (UPSC-CMS-2016) where the official answer key indicates A->2 B->1 C->4 D->3. While pairings A and B are medically accurate, pairings C and D have clinical inconsistencies that students should be aware of. *Incorrect A->2 B->1 C->3 D->4* - While correctly matching Nosocomial→Hepatitis B and Opportunistic→CMV - Incorrectly pairs Iatrogenic→Aplastic anemia and Epornithic→Influenza - Does not match the official answer key *Incorrect A->1 B->2 C->4 D->3* - Incorrectly pairs Nosocomial→CMV (though CMV can be nosocomial, Hepatitis B is the better match here) - Incorrectly pairs Opportunistic→Hepatitis B (not typically classified as opportunistic) - Does not match the official answer key *Incorrect A->1 B->2 C->3 D->4* - All pairings are incorrect - Does not match the official answer key
Question 30: With reference to International Certificate of Vaccination for Yellow Fever, the validity of the certificate begins how many days after the vaccination?
- A. 14 days
- B. 20 days
- C. 10 days (Correct Answer)
- D. 5 days
Explanation: ***10 days*** - The **International Certificate of Vaccination** for **yellow fever** becomes valid 10 days after the primary vaccination. This 10-day period aligns with the time needed for the immune system to develop a protective response. - This regulation ensures that individuals traveling to **yellow fever endemic areas** have sufficient immunity to prevent disease transmission and protect themselves. *14 days* - This is an incorrect timeframe; the specified waiting period for the **yellow fever vaccine** certificate to become valid is not 14 days. - While immune responses can develop over varying periods, the international regulation specifically states a shorter interval for certificate validity. *20 days* - This timeframe is longer than the internationally recognized period for the validity of the **yellow fever vaccination certificate** to commence. - A 20-day waiting period would cause unnecessary delays for travelers, as adequate protection is generally achieved earlier. *5 days* - Five days is too short a period for the body to mount a sufficient and recognized **immune response** to the **yellow fever vaccine**. - A shorter waiting period might lead to a false sense of security, as full protection may not yet be established, increasing the risk of infection.