UPSC-CMS 2016
114 Previous Year Questions with Answers & Explanations
Community Medicine
1 questionsIn India, the commonest cause of unilateral lymphoedema of lower limb is:
UPSC-CMS 2016 - Community Medicine UPSC-CMS Practice Questions and MCQs
Question 1: In India, the commonest cause of unilateral lymphoedema of lower limb is:
- A. Tubercular lymphadenopathy
- B. Filariasis (Correct Answer)
- C. Carcinoma of penis
- D. Lymphoedema tarda
Explanation: ***Filariasis (Correct Answer)*** - **Filariasis**, particularly caused by *Wuchereria bancrofti*, is endemic in many parts of India and is the leading cause of **secondary lymphedema** worldwide. - The parasitic worms block the lymphatic vessels, leading to chronic swelling, thickening of the skin, and can cause grotesque enlargement of limbs, often unilaterally. - In India, filariasis accounts for the vast majority of acquired unilateral lower limb lymphedema cases. *Tubercular lymphadenopathy (Incorrect)* - While **tubercular lymphadenopathy** is common in India, it primarily causes swelling of lymph nodes, often in the neck or axilla. - It typically does not lead to diffuse, unilateral lymphedema of the entire lower limb. *Carcinoma of penis (Incorrect)* - **Carcinoma of the penis** can cause inguinal lymph node metastasis, which might lead to lymphedema if the nodes are extensively involved or surgically removed. - However, it is not the most common cause of unilateral lower limb lymphedema in the general population of India. *Lymphoedema tarda (Incorrect)* - **Lymphedema tarda** is a form of primary lymphedema that typically presents after the age of 35, often without an identifiable cause. - While it can occur in India, it is a congenital or developmental disorder of the lymphatic system and is far less common than filariasis as a cause of acquired lymphedema.
Dermatology
1 questionsWhich of the following statements is not correct regarding sebaceous cyst?
UPSC-CMS 2016 - Dermatology UPSC-CMS Practice Questions and MCQs
Question 1: Which of the following statements is not correct regarding sebaceous cyst?
- A. Found on hairy areas of the body
- B. Treatment is incision and drainage (Correct Answer)
- C. Not found on palms and soles
- D. It has a punctum
Explanation: ***Treatment is incision and drainage*** - The standard treatment for a sebaceous cyst (more accurately an **epidermoid cyst** or **pilar cyst**) is **surgical excision** of the entire cyst wall to prevent recurrence. - **Incision and drainage** only provides temporary relief by emptying the contents but leaves the cyst wall intact, leading to a high chance of the cyst refilling. *Found on hairy areas of the body* - This statement is generally correct as sebaceous cysts often arise from hair follicles and are common in **hair-bearing areas** like the scalp, face, neck, and trunk. - They occur due to the accumulation of **sebum** and keratin within a blocked or damaged sebaceous gland or hair follicle. *Not found on palms and soles* - This statement is correct because **palms and soles** generally **lack sebaceous glands** and hair follicles, hence sebaceous cysts are typically not found in these locations. - Cysts found in these areas are more likely to be **ganglion cysts** or other types of epidermal inclusion cysts. *It has a punctum* - This statement is often correct; many sebaceous cysts (especially epidermoid cysts) have a visible **central punctum** which represents the occluded pore from which the cyst originated. - This punctum is a **key diagnostic feature** and can sometimes exude a cheesy, foul-smelling material.
Internal Medicine
4 questionsA patient has recurrent abdominal pain and jaundice. The blood investigations reveal reticulocytosis and hyperbilirubinemia. What is the clinical diagnosis?
The following conditions are associated with high incidence of pigment gallstones except:
The most common route of spread in a case of pyogenic liver abscess is:
The most common complication of pancreas divisum is:
UPSC-CMS 2016 - Internal Medicine UPSC-CMS Practice Questions and MCQs
Question 1: A patient has recurrent abdominal pain and jaundice. The blood investigations reveal reticulocytosis and hyperbilirubinemia. What is the clinical diagnosis?
- A. Hereditary spherocytosis (Correct Answer)
- B. Mirizzi's syndrome
- C. Sclerosing cholangitis
- D. Choledochal cyst
Explanation: ***Hereditary spherocytosis*** - The combination of **recurrent abdominal pain**, **jaundice**, **reticulocytosis**, and **hyperbilirubinemia** is highly suggestive of hereditary spherocytosis, which causes chronic hemolytic anemia [1, 3]. - **Jaundice** and **abdominal pain** can result from pigment gallstones (due to chronic hemolysis) and splenic enlargement, both common in this condition [2, 3]. *Mirizzi's syndrome* - Characterized by **extrinsic compression of the common hepatic duct** by a stone impacted in the cystic duct or gallbladder neck. - While it causes jaundice and abdominal pain, it does not typically present with **reticulocytosis** or **hemolysis** [1]. *Sclerosing cholangitis* - A chronic cholestatic liver disease characterized by **inflammation and fibrosis** of the bile ducts. - While it causes jaundice and abdominal pain, it is not associated with **reticulocytosis** or signs of **hemolysis** [1]. *Choledochal cyst* - A **congenital dilation of the bile ducts**, leading to recurrent abdominal pain, jaundice, and a palpable mass. - It does not involve **hemolysis** or **reticulocytosis**, making it less likely in this context.
Question 2: The following conditions are associated with high incidence of pigment gallstones except:
- A. Prosthetic heart valve (Correct Answer)
- B. Cirrhosis
- C. Thalassemia
- D. Ileal disease
Explanation: The following conditions are associated with high incidence of pigment gallstones except: ***Prosthetic heart valve*** - A prosthetic heart valve is not directly associated with an increased incidence of **pigment gallstones**. Conditions leading to pigment gallstones typically involve **hemolysis** or biliary stasis/infection. - While complications like endocarditis or hemolysis can occur with prosthetic valves, they are not a primary driver of pigment gallstone formation. *Cirrhosis* - **Cirrhosis** is associated with an increased risk of pigment gallstones due to altered bile composition and bile stasis. - The impaired liver function in cirrhosis leads to increased **bilirubin excretion** and precipitation. *Thalassemia* - **Thalassemia** is a hematologic disorder characterized by **chronic hemolysis**, which leads to an overload of unconjugated bilirubin. - This excess bilirubin is then excreted into the bile, increasing the risk of forming **pigment gallstones** [1]. *Ileal disease* - **Ileal disease** (e.g., Crohn's disease affecting the ileum, ileal resection) is primarily associated with an increased risk of **cholesterol gallstones**, not pigment gallstones. - Damage to the ileum impairs bile salt reabsorption, leading to a decreased bile salt pool and supersaturation of cholesterol in the bile.
Question 3: The most common route of spread in a case of pyogenic liver abscess is:
- A. Hepatic artery
- B. Ascending infection through biliary duct
- C. Local spread
- D. Haematogenous through portal vein (Correct Answer)
Explanation: Haematogenous through portal vein - Pyogenic liver abscesses commonly result from bacterial translocation from the gut, reaching the liver via the portal venous system. - This route accounts for a significant proportion of cases, especially when associated with conditions like diverticulitis or appendicitis. *Hepatic artery* - While possible, spread via the hepatic artery is less common and usually seen in cases of septicemia or endocarditis. - It would imply a more generalized systemic infection rather than a localized abdominal source. *Ascending infection through biliary duct* - This mechanism is characteristic of cholangitis and often leads to multiple small abscesses or a subcapsular collection, not typically a solitary pyogenic liver abscess. - It occurs due to obstruction to biliary flow from stones or strictures. *Local spread* - Local spread can occur from adjacent infected organs like a subphrenic abscess or an infected gallbladder, but it is not the most common route for the initial development of a pyogenic liver abscess. - This typically results in direct extension into the liver parenchyma.
Question 4: The most common complication of pancreas divisum is:
- A. Obstructive jaundice
- B. Peptic ulcer
- C. Recurrent acute pancreatitis (Correct Answer)
- D. Duodenal obstruction
Explanation: ***Recurrent acute pancreatitis*** - **Pancreas divisum** is a congenital anomaly where the dorsal and ventral pancreatic ducts fail to fuse, leading to the **majority of pancreatic secretions draining through the smaller, narrower minor papilla**. - This anatomical variation can cause relative **obstruction to pancreatic exocrine flow**, particularly during periods of increased secretion, predisposing to **recurrent episodes of acute pancreatitis** [1]. *Obstructive jaundice* - **Obstructive jaundice** typically results from **biliary tract obstruction**, such as gallstones or tumors, affecting the common bile duct. - While pancreatic disease can cause jaundice, **pancreas divisum primarily affects the pancreatic duct system** and is not a common direct cause of biliary obstruction. *Peptic ulcer* - **Peptic ulcers** are lesions in the lining of the stomach or duodenum, usually caused by **_H. pylori_ infection** or **NSAID use**. - There is **no direct causal relationship** between pancreas divisum and the development of peptic ulcers. *Duodenal obstruction* - **Duodenal obstruction** can result from various causes such as **mass lesions (_e.g._, pancreatic head tumor), strictures, or malrotation**. - Pancreas divisum is an **anatomical variation of the pancreatic ducts**, and it does not directly cause mechanical obstruction of the duodenum itself.
Pathology
1 questionsMatch List-I with List-II and select the correct answer using the code given below the Lists:
UPSC-CMS 2016 - Pathology UPSC-CMS Practice Questions and MCQs
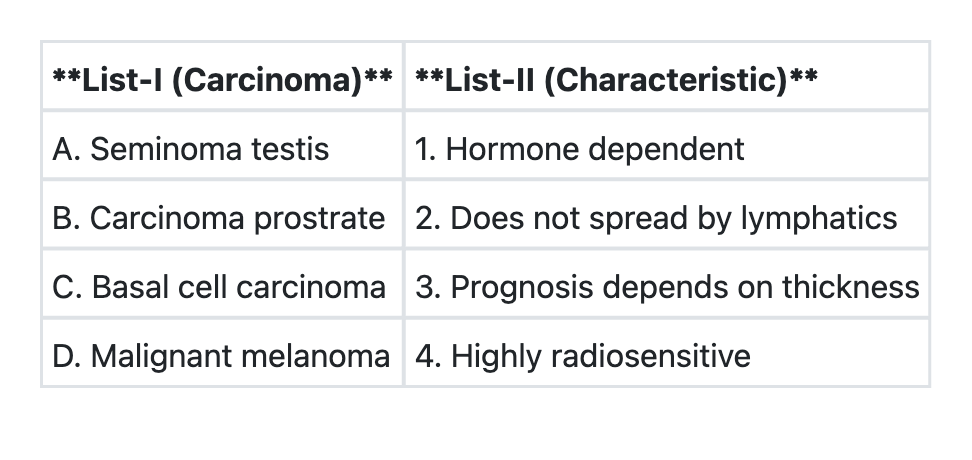
Question 1: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→4 B→1 C→2 D→3 (Correct Answer)
- B. A→3 B→2 C→1 D→4
- C. A→3 B→1 C→2 D→4
- D. A→4 B→2 C→1 D→3
Explanation: ***A→4 B→1 C→2 D→3*** - This option correctly matches each carcinoma with its characteristic feature. **Seminoma testis** is **highly radiosensitive** (A→4), making radiation therapy an effective treatment modality with excellent cure rates. **Carcinoma of the prostate** is **hormone-dependent** (B→1), relying on androgens for growth, which is why androgen deprivation therapy is a key treatment [1]. **Basal cell carcinoma** is a locally invasive tumor that **does not significantly spread by lymphatics** (C→2), which contributes to its excellent prognosis despite being the most common skin cancer [2, 4]. **Malignant melanoma** has a prognosis that depends on **Breslow thickness** (D→3), which measures the depth of invasion and is the most important prognostic factor. *A→4 B→2 C→1 D→3* - This option incorrectly states that **carcinoma of the prostate does not spread by lymphatics** (B→2) and that **basal cell carcinoma is hormone-dependent** (C→1). Prostate cancer commonly metastasizes to pelvic lymph nodes via lymphatic spread [1], and BCC is not influenced by hormones. *A→3 B→2 C→1 D→4* - This option incorrectly matches **seminoma testis** with prognosis depending on thickness (A→3) and **malignant melanoma** with being highly radiosensitive (D→4). Seminoma is radiosensitive (not melanoma), and melanoma's prognosis depends on Breslow thickness (not seminoma). *A→3 B→1 C→2 D→4* - This option correctly identifies that **prostate cancer is hormone-dependent** (B→1) and **basal cell carcinoma has limited lymphatic spread** (C→2), but incorrectly associates **seminoma testis** with prognosis depending on thickness (A→3) and **malignant melanoma** with being highly radiosensitive (D→4). These last two matches are reversed. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lower Urinary Tract and Male Genital System, pp. 993-994. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Skin, pp. 1157-1160. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Disorders Involving Inflammatory And Haemopoietic Cells, pp. 643-644.
Surgery
3 questionsTumours of anterior mediastinum include the following except:
Nottingham prognostic Index is used for:
In gallstone ileus, obstruction most frequently occurs at:
UPSC-CMS 2016 - Surgery UPSC-CMS Practice Questions and MCQs
Question 1: Tumours of anterior mediastinum include the following except:
- A. Lymphoma
- B. Germ cell tumour
- C. Thymoma
- D. Schwannoma (Correct Answer)
Explanation: ***Schwannoma*** - **Schwannomas** (neurilemmomas) are typically found in the **posterior mediastinum**, arising from **peripheral nerves** or nerve roots. - They are usually benign and grow slowly, presenting with symptoms due to compression of surrounding structures. *Lymphoma* - **Lymphoma** is a common tumor of the **anterior mediastinum**, often presenting as an **anterior mediastinal mass**. - Both Hodgkin and non-Hodgkin lymphomas can involve mediastinal lymph nodes. *Germ cell tumour* - **Germ cell tumors**, including **teratomas** and **seminomas**, frequently occur in the **anterior mediastinum**. - They arise from ectopic germ cell rests that migrate aberrantly during embryonic development. *Thymoma* - **Thymomas** are the most common primary tumor of the **anterior mediastinum**, originating from the **thymus gland**. - They are often associated with **myasthenia gravis** and other paraneoplastic syndromes.
Question 2: Nottingham prognostic Index is used for:
- A. Cancer stomach
- B. Cancer breast (Correct Answer)
- C. Cancer colon
- D. Cancer lung
Explanation: ***Cancer breast*** - The **Nottingham Prognostic Index (NPI)** is a well-established tool used specifically for assessing the prognosis of **early invasive breast cancer**. - It combines three key pathological features: **tumor size**, **lymph node status**, and **histological grade**, to provide a prognostic score. *Cancer stomach* - Prognostic indices for gastric cancer typically involve factors like **tumor depth (T stage)**, **lymph node involvement (N stage)**, **metastasis (M stage)**, and **histological type**. - The NPI is not validated or used for gastric cancer. *Cancer colon* - Prognosis in colorectal cancer is primarily determined by the **Dukes' staging system** or the **TNM staging system**, which consider tumor invasion depth, lymph node spread, and distant metastasis. - The NPI is not applicable to colorectal cancer. *Cancer lung* - Lung cancer prognosis depends heavily on the **TNM staging system**, differentiating between **non-small cell lung cancer** and **small cell lung cancer**, and considering factors like tumor size, nodal involvement, and metastases. - There is no role for the NPI in assessing lung cancer prognosis.
Question 3: In gallstone ileus, obstruction most frequently occurs at:
- A. Jejunum
- B. Duodenum
- C. Terminal ileum (Correct Answer)
- D. Proximal ileum
Explanation: ***Terminal ileum*** - In gallstone ileus, the **terminal ileum** (particularly at the **ileocecal valve region**) is the most common site of obstruction, accounting for **60-70%** of cases. - This occurs because the terminal ileum is the **narrowest portion of the small bowel**, creating a natural anatomical bottleneck where large gallstones become impacted. - The **ileocecal valve** represents the point of transition from small to large bowel, and its relatively fixed position and narrow caliber make it the classic site of obstruction. *Proximal ileum* - While gallstones can cause obstruction in the proximal or mid-ileum, this is **less frequent** than terminal ileum obstruction. - The proximal ileum has a relatively wider lumen compared to the terminal ileum, allowing larger stones to pass through more easily. *Jejunum* - The **jejunum** has the widest lumen of the small bowel, making obstruction at this site uncommon. - Gallstones typically pass through the jejunum without causing impaction. *Duodenum* - Duodenal obstruction by a gallstone is called **Bouveret's syndrome** and represents a rare variant (1-4% of gallstone ileus cases). - This occurs when a large stone impacts in the duodenal bulb or pylorus after eroding through a cholecystoduodenal fistula.
About UPSC-CMS 2016 Questions
This page contains 114 questions from the UPSC-CMS 2016 paper, organised across 13 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the UPSC-CMS exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your UPSC-CMS goals.