All SubjectsAnatomy (12)Anesthesiology (3)Biochemistry (13)Community Medicine (15)Dermatology (3)ENT (6)Forensic Medicine (7)General Medicine (1)Internal Medicine (28)Microbiology (10)Obstetrics and Gynecology (16)Ophthalmology (6)Orthopaedics (2)Pathology (17)Pediatrics (3)Pharmacology (8)Physiology (5)Psychiatry (7)Radiology (6)Surgery (8)
Q11
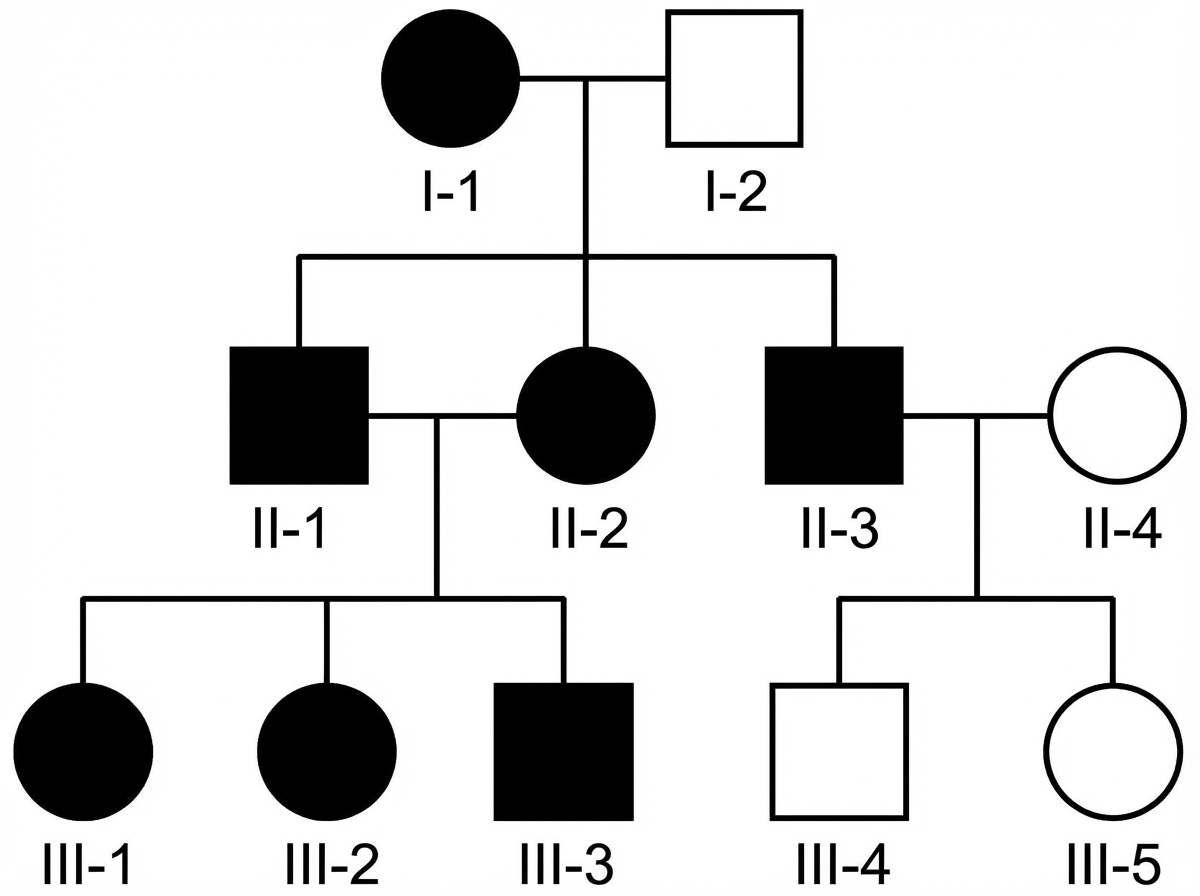
The pedigree chart shown in the image demonstrates a specific pattern of inheritance. Which of the following conditions is most likely to follow this pattern of inheritance?
Q12
A middle-aged man from an endemic region presents with progressive swelling of the lower limb. A peripheral blood smear shows the following structure. What is the most likely cause of his limb swelling?
Q13
A 45-year-old female presents with a 2-year history of progressive unilateral hearing loss, tinnitus, and unsteadiness. An MRI scan reveals a well-defined tumor located in the cerebellopontine angle (CPA). A surgical resection is performed, and subsequent histopathological examination of the tumor tissue is given below. Based on these histopathological findings, what is the most likely diagnosis?
Q14
A 15-year-old tall boy with long limbs presents to the OPD. On ocular examination, bilateral ectopia lentis is noted. Which gene is most likely affected in this inherited disorder?
Q15
A 25-year old patient who had a Road traffic accident was initially conscious but later became unconscious and subsequently died. On postmortem examination, multiple petechial hemorrhages are seen in the corpus callosum, what is the probable diagnosis?
Q16
A patient presents with morning stiffness and tests positive for anti-CCP antibodies. Which of the following histological features is most characteristic of the underlying disease?
Q17
Patient presents with dry cough, dyspnea and stridor. HPE of hilar LN shows stellate granulomas with giant cells and circular lamellated concretions on histopathology. Which of the following is the most likely diagnosis?