All (177)Anatomy (12)Anesthesiology (3)Biochemistry (13)Community Medicine (15)Dermatology (3)ENT (6)Forensic Medicine (7)General Medicine (1)Internal Medicine (28)Microbiology (10)Obstetrics and Gynecology (16)Ophthalmology (6)Orthopaedics (2)Pathology (17)Pediatrics (3)Pharmacology (8)Physiology (5)Psychiatry (7)Radiology (6)Surgery (9)
Q51
A 68-year-old man presents with bleeding manifestations. Peripheral smear shows the presence of cells shown below. Which of the following is the most common chromosomal abnormality seen in this condition?
Q52
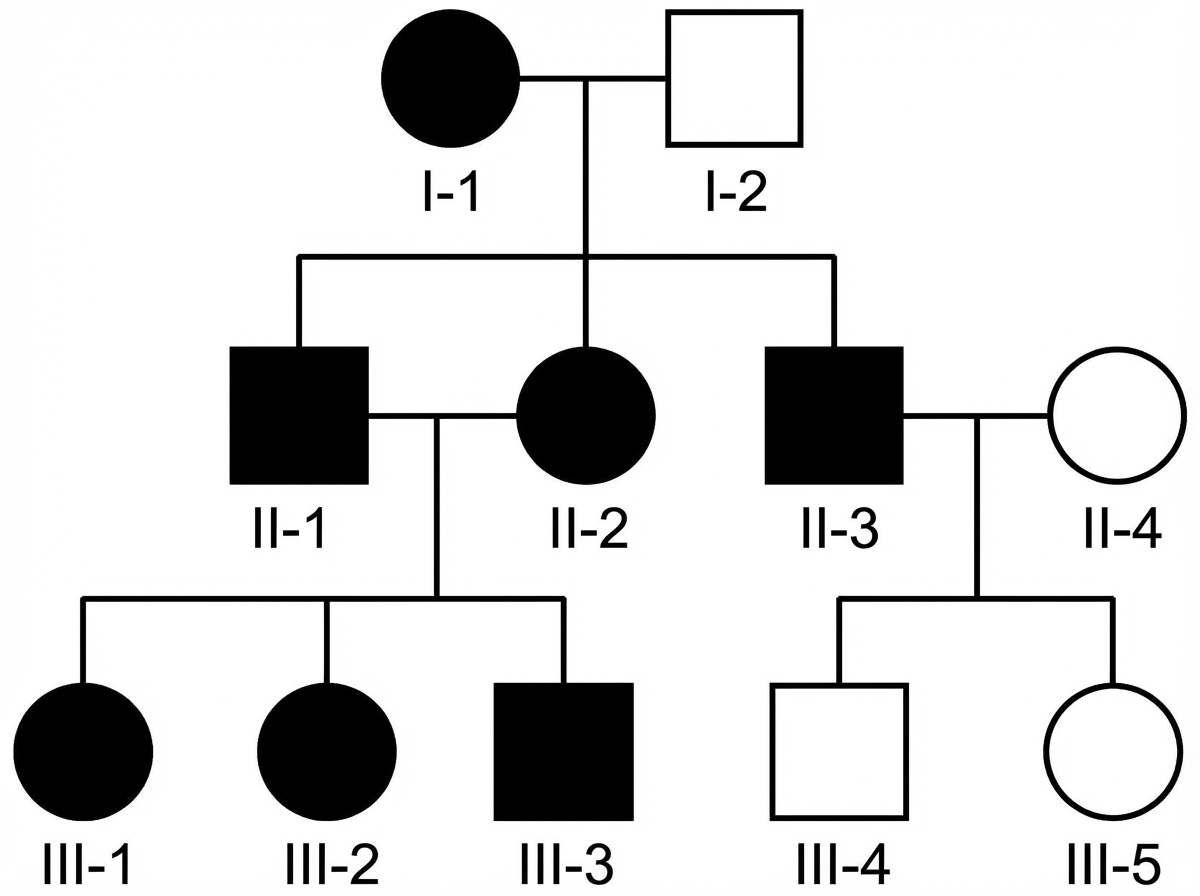
The pedigree chart shown in the image demonstrates a specific pattern of inheritance. Which of the following conditions is most likely to follow this pattern of inheritance?