All (176)Anatomy (12)Anesthesiology (3)Biochemistry (13)Community Medicine (15)Dermatology (3)ENT (6)Forensic Medicine (7)General Medicine (1)Internal Medicine (28)Microbiology (10)Obstetrics and Gynecology (16)Ophthalmology (6)Orthopaedics (2)Pathology (17)Pediatrics (3)Pharmacology (8)Physiology (5)Psychiatry (7)Radiology (6)Surgery (8)
Q21
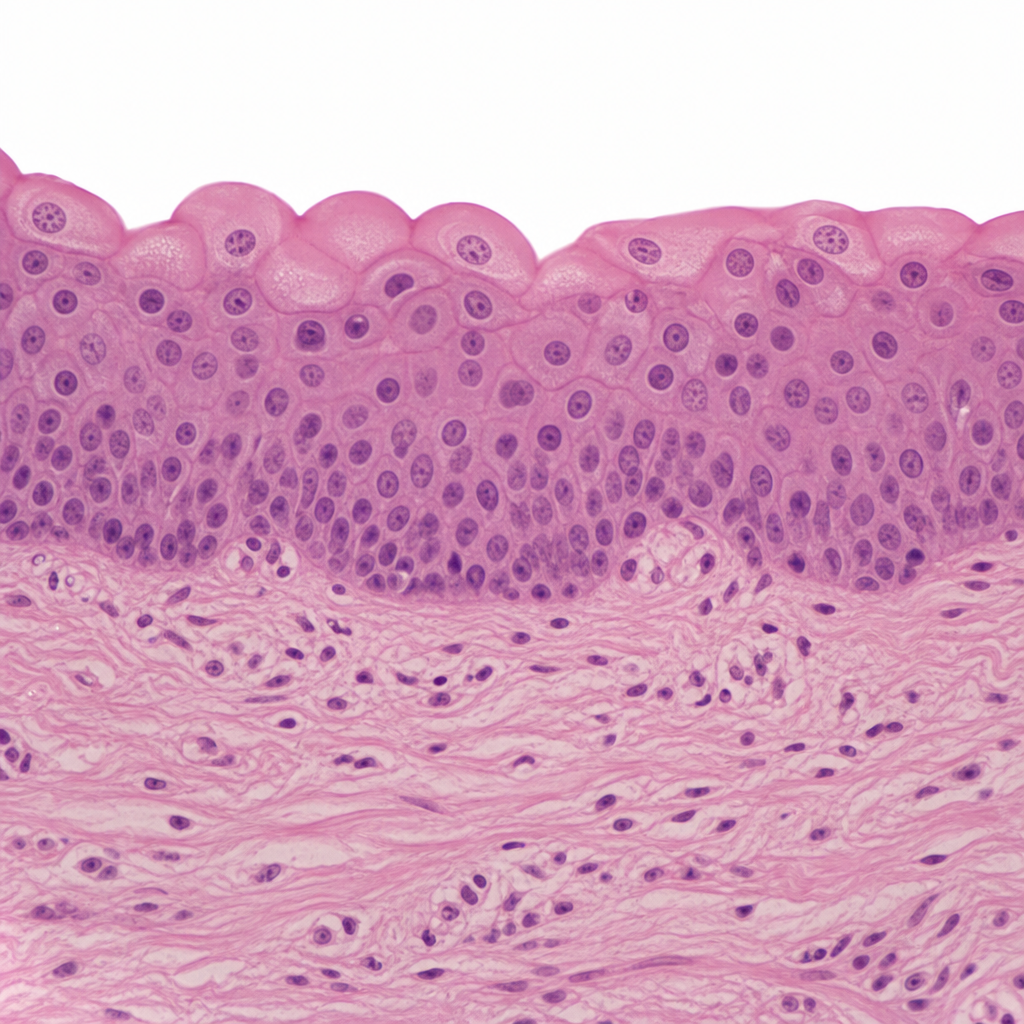
This type of epithelium is most likely found lining which of the following structures?