All (177)Anatomy (12)Anesthesiology (3)Biochemistry (13)Community Medicine (15)Dermatology (3)ENT (6)Forensic Medicine (7)General Medicine (1)Internal Medicine (28)Microbiology (10)Obstetrics and Gynecology (16)Ophthalmology (6)Orthopaedics (2)Pathology (17)Pediatrics (3)Pharmacology (8)Physiology (5)Psychiatry (7)Radiology (6)Surgery (9)
Q141
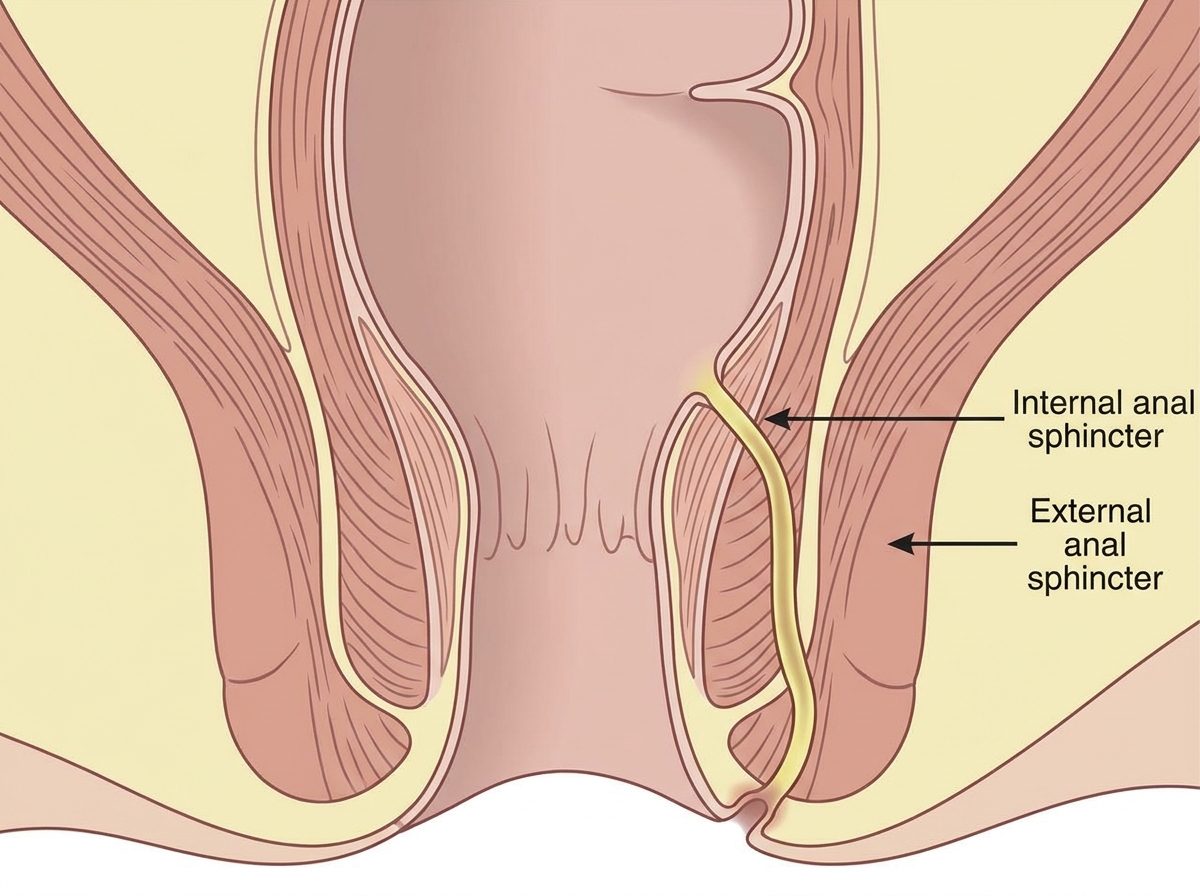
What is the most probable diagnosis based on the image provided?
Q142
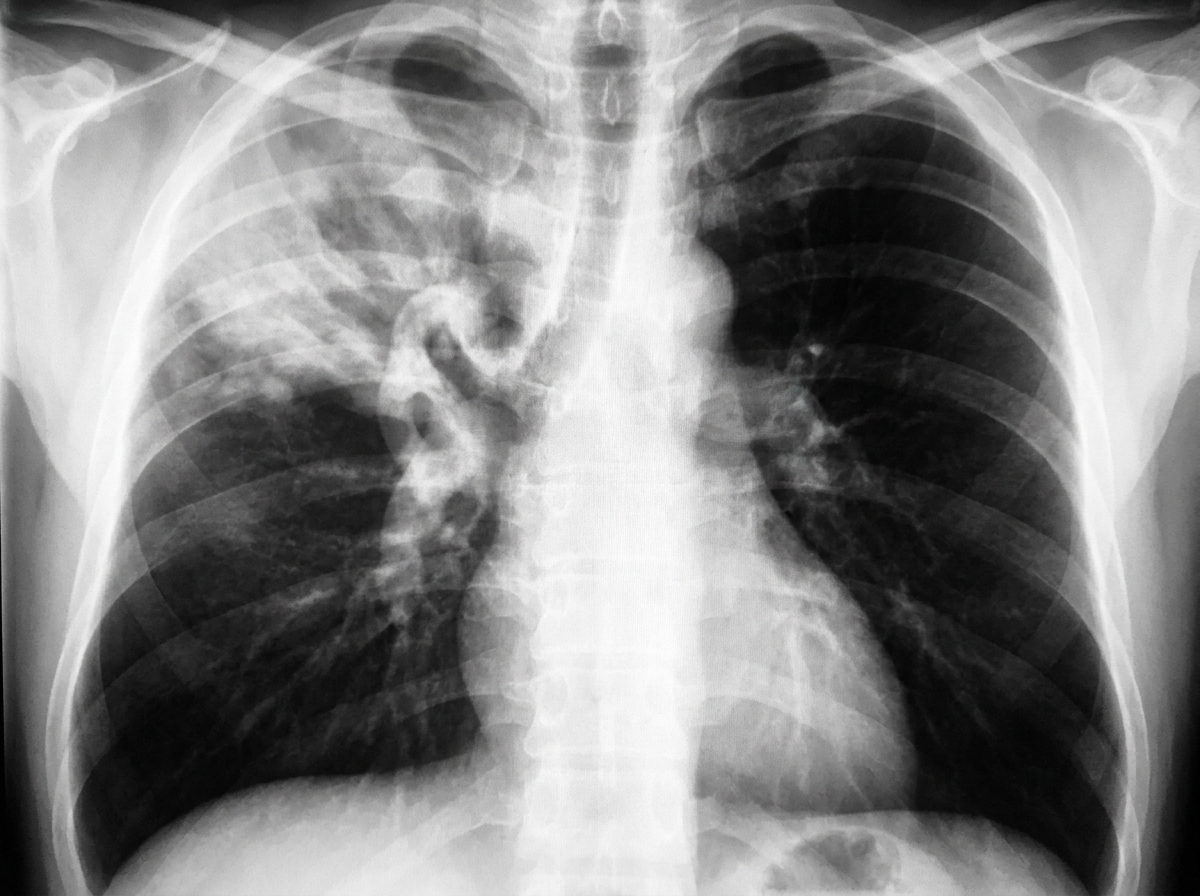
Which is the earliest imaging modality used to detect ankylosing spondylitis?