All (176)Anatomy (12)Anesthesiology (3)Biochemistry (13)Community Medicine (15)Dermatology (3)ENT (6)Forensic Medicine (7)General Medicine (1)Internal Medicine (28)Microbiology (10)Obstetrics and Gynecology (16)Ophthalmology (6)Orthopaedics (2)Pathology (17)Pediatrics (3)Pharmacology (8)Physiology (5)Psychiatry (7)Radiology (6)Surgery (8)
Q101
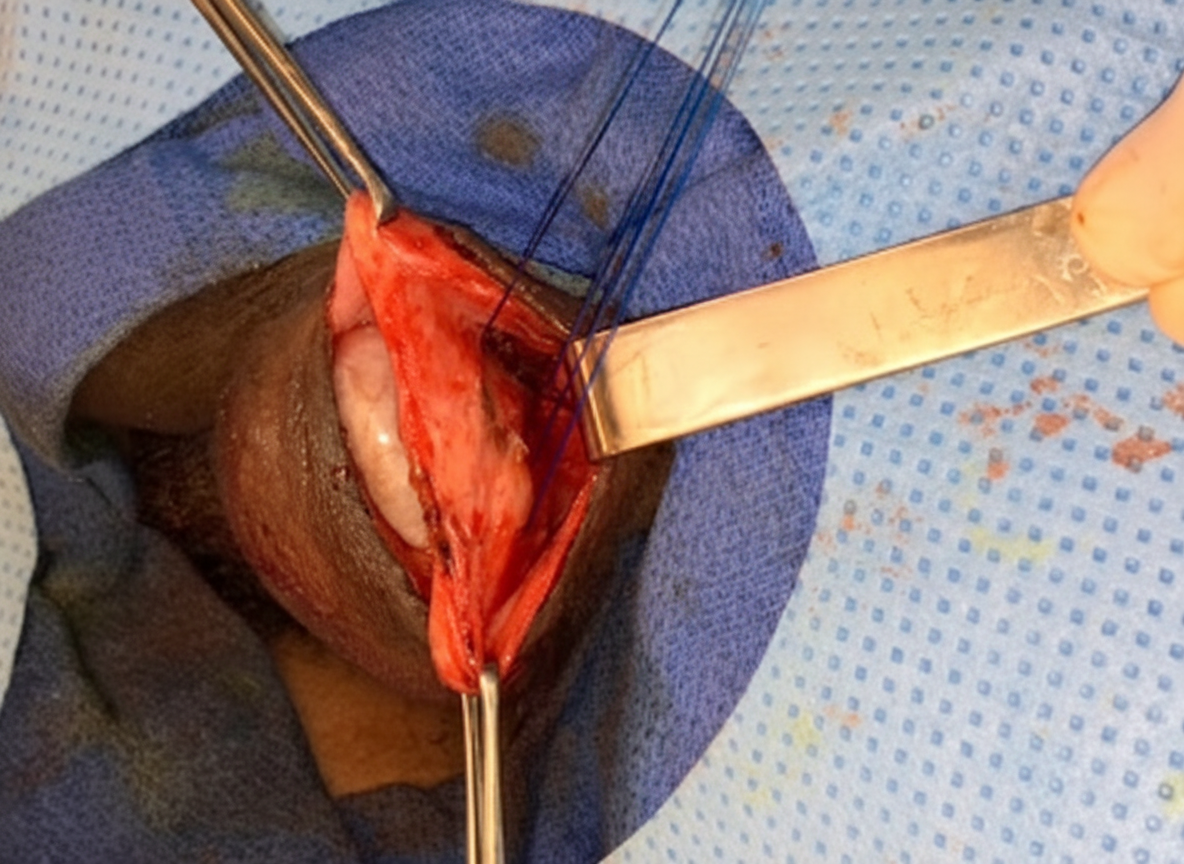
What is correct regarding this suture?
Q102
History of pulsatile mass in the neck. Digital angiography image shown. Not filling on carotid compression. But refilling on releasing pressure. What is the diagnosis?