The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?
Q2
The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?
Q3
The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?
Q4
The image shows a congenital cardiac defect. Abnormal development of which branch of aortic arch leads to this defect?
Q5
During a neck dissection, a nerve was identified and marked that is most likely the vagus nerve (CN X). Which of the following is NOT a functional component of the vagus nerve?
Q6
What is the correct nerve supply to the muscles labelled as A and B ?
Q7
A patient presents with meralgia paresthetica. Based on the diagram, identify the nerve involved in this condition.
NEET-PG 2025 - Anatomy NEET-PG Practice Questions and MCQs
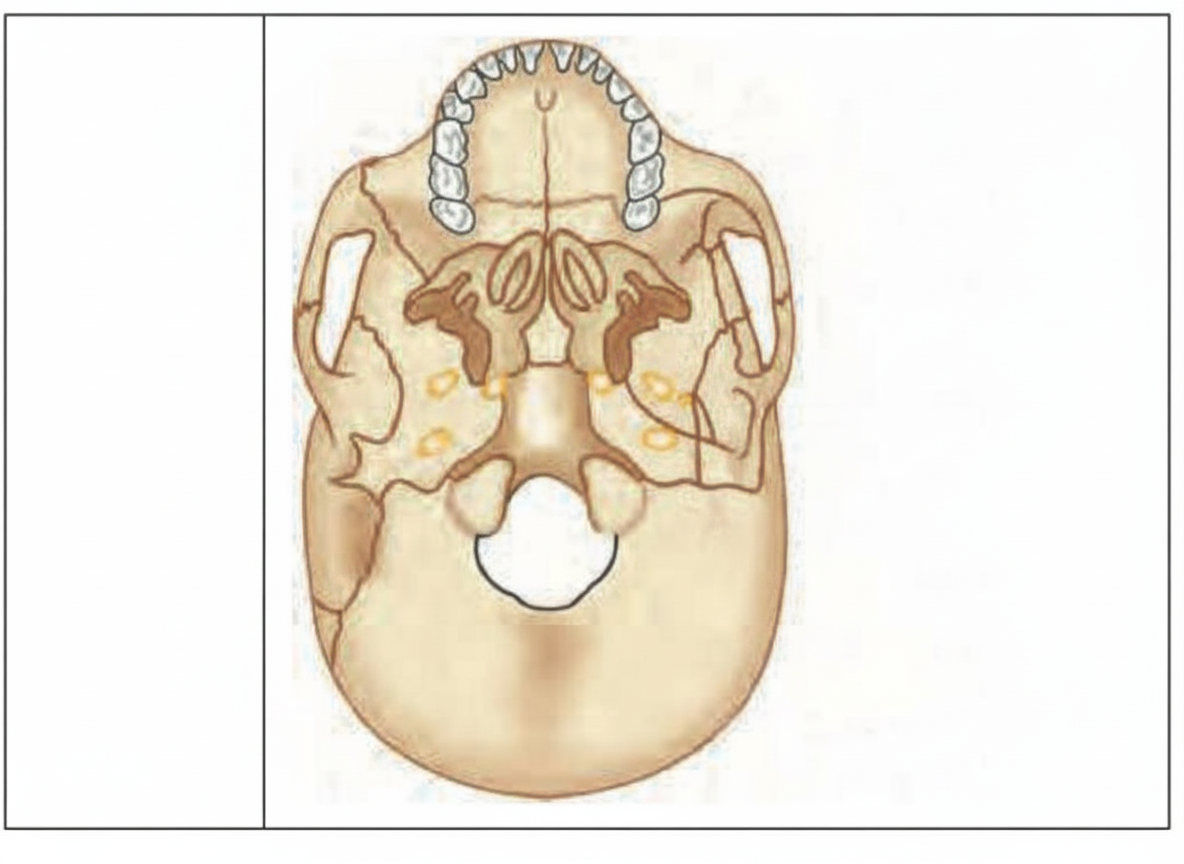
Question 1: The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?
A. Hypoglossal nerve (Correct Answer)
B. Accessory nerve
C. Glossopharyngeal nerve
D. Vagus nerve
Explanation: ***Hypoglossal nerve***
- The **Hypoglossal nerve (CN XII)** does not pass through the jugular foramen; instead, it utilizes a distinct opening called the **Hypoglossal canal**.
- This canal is found in the **occipital bone**, separate from the structures passing through the jugular foramen.
*Accessory nerve*
- The **Accessory nerve (CN XI)** is one of the three cranial nerves (IX, X, XI) that pass through the jugular foramen.
- It provides motor supply to the **sternocleidomastoid** and **trapezius muscles**.
*Glossopharyngeal nerve*
- The **Glossopharyngeal nerve (CN IX)** exits the skull through the anterior part of the jugular foramen.
- It is known for innervating the **stylopharyngeus muscle** and carrying sensation and taste from the posterior one-third of the tongue.
*Vagus nerve*
- The **Vagus nerve (CN X)** passes through the jugular foramen, primarily through its middle compartment.
- It is the major parasympathetic nerve supplying the **thorax and abdomen**, as well as motor supply to the **larynx** and pharynx.
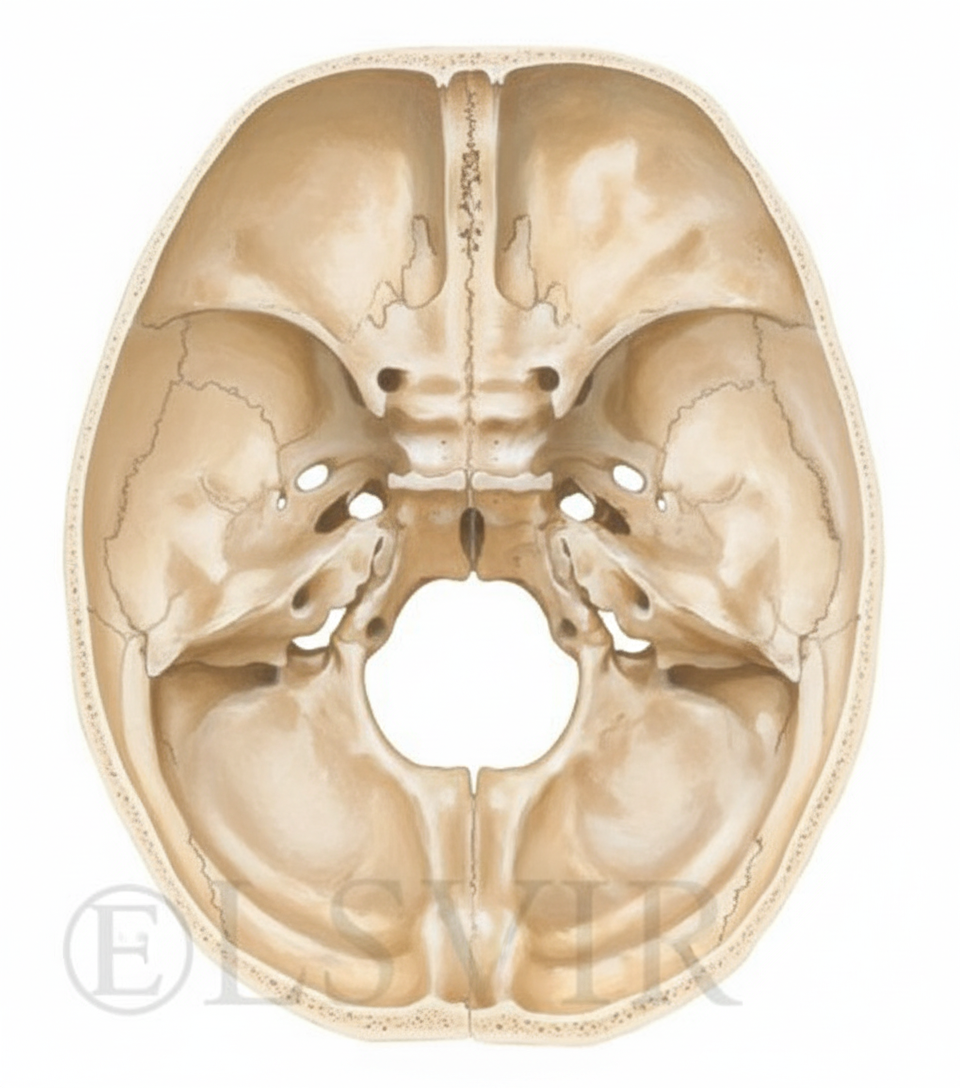
Question 2: The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?
A. Hypoglossal nerve (Correct Answer)
B. Accessory nerve
C. Glossopharyngeal nerve
D. Vagus nerve
Explanation: ***Hypoglossal nerve***
- The **Hypoglossal nerve (CN XII)** does not pass through the jugular foramen; instead, it utilizes a distinct opening called the **Hypoglossal canal**.
- This canal is found in the **occipital bone**, separate from the structures passing through the jugular foramen.
*Accessory nerve*
- The **Accessory nerve (CN XI)** is one of the three cranial nerves (IX, X, XI) that pass through the jugular foramen.
- It provides motor supply to the **sternocleidomastoid** and **trapezius muscles**.
*Glossopharyngeal nerve*
- The **Glossopharyngeal nerve (CN IX)** exits the skull through the anterior part of the jugular foramen.
- It is known for innervating the **stylopharyngeus muscle** and carrying sensation and taste from the posterior one-third of the tongue.
*Vagus nerve*
- The **Vagus nerve (CN X)** passes through the jugular foramen, primarily through its middle compartment.
- It is the major parasympathetic nerve supplying the **thorax and abdomen**, as well as motor supply to the **larynx** and pharynx.
Question 3: The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?
A. Hypoglossal nerve (Correct Answer)
B. Accessory nerve
C. Glossopharyngeal nerve
D. Vagus nerve
Explanation: ***Hypoglossal nerve***
- The **Hypoglossal nerve (CN XII)** does not pass through the jugular foramen; instead, it utilizes a distinct opening called the **Hypoglossal canal**.
- This canal is found in the **occipital bone**, separate from the structures passing through the jugular foramen.
*Accessory nerve*
- The **Accessory nerve (CN XI)** is one of the three cranial nerves (IX, X, XI) that pass through the jugular foramen.
- It provides motor supply to the **sternocleidomastoid** and **trapezius muscles**.
*Glossopharyngeal nerve*
- The **Glossopharyngeal nerve (CN IX)** exits the skull through the anterior part of the jugular foramen.
- It is known for innervating the **stylopharyngeus muscle** and carrying sensation and taste from the posterior one-third of the tongue.
*Vagus nerve*
- The **Vagus nerve (CN X)** passes through the jugular foramen, primarily through its middle compartment.
- It is the major parasympathetic nerve supplying the **thorax and abdomen**, as well as motor supply to the **larynx** and pharynx.
Question 4: The image shows a congenital cardiac defect. Abnormal development of which branch of aortic arch leads to this defect?
A. Right 6th aortic arch
B. Left 6th aortic arch (Correct Answer)
C. Left 4th aortic arch
D. Right 4th aortic arch
Explanation: ***Left 6th aortic arch***
- The **Ductus Arteriosus**, which shunts blood from the pulmonary artery to the aorta in fetal life, is embryologically derived from the distal portion of the **Left 6th Aortic Arch**.
- **Patent Ductus Arteriosus (PDA)** is the failure of this fetal connection to close after birth.
*Right 4th aortic arch*
- The **Right 4th Aortic Arch** contributes to the formation of the proximal segment of the **Right Subclavian Artery**.
- Defects in the right 4th arch are typically associated with vascular ring anomalies, such as an aberrant right subclavian artery.
*Right 6th aortic arch*
- The **Right 6th Aortic Arch** forms the proximal segment of the **Right Pulmonary Artery**.
- The distal part of the right 6th arch normally involutes and disappears completely, unlike the persistence seen on the left side (PDA).
*Left 4th aortic arch*
- The **Left 4th Aortic Arch** forms the segment of the **Arch of the Aorta** located between the left common carotid and the left subclavian arteries.
- This arch is primarily involved in forming the main aortic arch structure.
Question 5: During a neck dissection, a nerve was identified and marked that is most likely the vagus nerve (CN X). Which of the following is NOT a functional component of the vagus nerve?
A. General visceral afferent
B. General somatic efferent (Correct Answer)
C. General visceral efferent
D. General somatic afferent
Explanation: ***General somatic efferent***
- **GSE** fibers innervate muscles derived from **somites**, typically cranial nerves that control the extraocular muscles (CN III, IV, VI) or the tongue muscles (CN XII).
- The vagus nerve (CN X) does not carry GSE fibers; its motor components are **Special Visceral Efferent (SVE)** for pharyngeal/laryngeal muscles, and **General Visceral Efferent (GVE)** for parasympathetic supply.
*General visceral afferent*
- **GVA** fibers are a major functional component of the vagus nerve, providing **visceral sensation** from the respiratory, cardiovascular, and gastrointestinal systems.
- These fibers monitor stretch receptors in the lungs, **baroreceptors** in the aortic arch, and sensation from the abdominal viscera, crucial for reflex regulation.
*General visceral efferent*
- **GVE** fibers represent the **parasympathetic outflow** of the vagus nerve below the neck, innervating smooth muscle, cardiac muscle, and glands.
- This component is responsible for decreasing **heart rate**, promoting **bronchoconstriction**, and increasing gastrointestinal motility and secretion.
*General somatic afferent*
- **GSA** fibers carry general sensory information (pain, temperature, touch) from parts of the head and are present in the vagus nerve.
- CN X GSA fibers provide sensation from a small area of the external auditory meatus and the external surface of the **tympanic membrane**.
Question 6: What is the correct nerve supply to the muscles labelled as A and B ?
A. A - Facial nerve, B - Spinal accessory nerve
B. A - Spinal accessory nerve, B - Mandibular nerve
C. A - Facial nerve, B - Nerve to mylohyoid
D. A - Mandibular nerve, B - Facial nerve (Correct Answer)
Explanation: ***A - Mandibular nerve, B - Facial nerve***
- Label A points to the **Masseter** muscle, which is supplied by the **Mandibular nerve (V3)** via the masseteric nerve.
- Label B points to the **Platysma** muscle, which is a muscle of facial expression supplied by the **Facial nerve (VII)** via the cervical branch.
*A - Facial nerve, B - Nerve to mylohyoid*
- The **Masseter** (A) is a muscle of mastication supplied by the **Mandibular nerve (V3)**, not the facial nerve.
- The **Nerve to mylohyoid** supplies the mylohyoid muscle and anterior belly of digastric, whereas B is the **Platysma** muscle supplied by the facial nerve.
*A - Facial nerve, B - Spinal accessory nerve*
- The **Facial nerve (VII)** supplies muscles of facial expression, not muscles of mastication like the **Masseter** (A).
- The **Spinal accessory nerve (XI)** supplies the sternocleidomastoid and trapezius muscles; it does not supply the **Platysma** (B).
*A - Spinal accessory nerve, B - Mandibular nerve*
- The **Masseter** (A) is supplied by the **Mandibular nerve (V3)**, not the spinal accessory nerve (XI).
- The **Platysma** (B) is supplied by the **Facial nerve (VII)**, not the mandibular nerve (V3).
Question 7: A patient presents with meralgia paresthetica. Based on the diagram, identify the nerve involved in this condition.
A. A
B. B
C. C (Correct Answer)
D. D
Explanation: ***C (Lateral Femoral Cutaneous Nerve)***
- Meralgia paresthetica is an entrapment neuropathy caused by compression of the **Lateral Femoral Cutaneous Nerve (LFCN)**, which corresponds to C in the diagram and arises from **L2 and L3** roots.
- Compression usually occurs as the nerve passes under the **inguinal ligament**, resulting in pain, numbness, and tingling over the **anterolateral thigh**.
*A (Ilioinguinal/Iliohypogastric Nerve)*
- Nerve A, usually the Ilioinguinal or Iliohypogastric nerve (T12, L1), innervates the **inguinal region** and lower abdominal wall.
- Entrapment of these nerves results in pain radiating towards the **groin** or superior thigh, not the characteristic distribution of meralgia paresthetica.
*B (Genitofemoral Nerve)*
- Nerve B is the **Genitofemoral nerve** (L1, L2), which supplies sensation to the superior medial thigh and genitalia.
- Injury results in loss of the **cremasteric reflex** and sensory changes in the scrotal/labial and proximal anterior thigh area.
*D (Femoral Nerve)*
- Nerve D is the large **Femoral Nerve** (L2-L4), responsible for motor supply to the **quadriceps** and sensation to the anterior thigh and medial leg.
- Compression typically causes prominent **quadriceps weakness** (difficulty extending the knee) in addition to sensory loss, unlike the purely sensory presentation of meralgia paresthetica.
Biochemistry
1 questions
Q1
A child presents with a history of fractures, multiple petechiae, perifollicular hemorrhages, and gum bleeding. Which of the following enzyme defects is involved?
NEET-PG 2025 - Biochemistry NEET-PG Practice Questions and MCQs
Question 1: A child presents with a history of fractures, multiple petechiae, perifollicular hemorrhages, and gum bleeding. Which of the following enzyme defects is involved?
A. Tyrosinase
B. Prolyl hydroxylase (Correct Answer)
C. Alkaline phosphatase
D. Lysyl oxidase
Explanation: ***Prolyl hydroxylase***
- **Vitamin C (Ascorbic acid)** is a necessary cofactor for Prolyl hydroxylase and Lysyl hydroxylase, which are essential for the hydroxylation of proline and lysine residues in procollagen.
- Deficiency of Vitamin C leads to inactivation of this enzyme, resulting in unstable and defective **collagen** that causes vascular fragility (leading to petechiae and gum bleeding) and impaired bone matrix (resulting in fractures).
*Lysyl oxidase*
- **Lysyl oxidase** is required for the crucial cross-linking of collagen and elastin fibers, a process that relies on **copper**, not Vitamin C, as a main cofactor.
- A defect in this enzyme primarily causes syndromes like certain types of **Ehlers-Danlos Syndrome** (Type V) or features associated with **Menkes disease**.
*Tyrosinase*
- **Tyrosinase** is the key enzyme in the biosynthesis of **melanin** from tyrosine.
- A defect in Tyrosinase causes various forms of **Albinism**, characterized by lack of pigmentation in the skin, hair, and eyes, which is unrelated to the described hemorrhagic and skeletal findings.
*Alkaline phosphatase*
- **Alkaline phosphatase (ALP)** plays a vital role in bone mineralization by hydrolyzing pyrophosphate, preventing its inhibitory effect on calcification.
- While important for bone health, ALP deficiency causes **Hypophosphatasia**, and it is not directly involved in the pathogenesis of structural collagen defects seen in **Scurvy**.
Internal Medicine
1 questions
Q1
A 40-year-old man presents with discomfort in one of his joints. Synovial fluid aspiration reveals rhomboid-shaped, positively birefringent crystals under polarized light microscopy. Which of the following is the most likely diagnosis?
NEET-PG 2025 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 1: A 40-year-old man presents with discomfort in one of his joints. Synovial fluid aspiration reveals rhomboid-shaped, positively birefringent crystals under polarized light microscopy. Which of the following is the most likely diagnosis?
A. A. Gout
B. B. Rheumatoid arthritis
C. C. Pseudogout (Correct Answer)
D. D. Osteoarthritis
Explanation: ### Pseudogout
- Pseudogout, or **Calcium Pyrophosphate Dihydrate (CPPD) crystal deposition disease**, is classically identified by the presence of **rhomboid-shaped** crystals [1].
- These CPPD crystals exhibit **positive birefringence** under polarized light microscopy, a distinguishing feature from gout [1].
*Gout*
- Gout is characterized by monosodium urate (MSU) crystals, which are **needle-shaped**, not rhomboid [1].
- MSU crystals show **strong negative birefringence**, appearing yellow when aligned parallel to the compensator axis (Yellow parallel) [1].
*Rheumatoid arthritis*
- The primary diagnostic finding in rheumatoid arthritis (RA) synovial fluid is **inflammatory changes** (high WBC count, mostly neutrophils) and not the presence of crystals.
- RA is associated with **RF** and **anti-CCP antibodies** and primarily affects smaller joints symmetrically.
*Osteoarthritis*
- Osteoarthritis (OA) synovial fluid is typically **non-inflammatory**, appearing viscous with a low white blood cell count (<2000 cells/mm³).
- OA is a degenerative joint disease defined by **cartilage loss** and **osteophyte formation**, not crystal deposition [1].
Orthopaedics
1 questions
Q1
A Patients presents with ankle pain and swelling after a forceful eversion injury. Based on the mechanism of injury, which ligament is most likely to be damaged?
NEET-PG 2025 - Orthopaedics NEET-PG Practice Questions and MCQs
Question 1: A Patients presents with ankle pain and swelling after a forceful eversion injury. Based on the mechanism of injury, which ligament is most likely to be damaged?
A. Posterior talofibular ligament
B. Anterior talofibular ligament
C. Deltoid ligament (Correct Answer)
D. Calcaneofibular ligament
Explanation: ***Deltoid ligament***- This strong ligament complex is located on the medial side of the ankle and is the primary stabilizer resisting excessive **valgus** or **eversion forces**.- A forceful eversion mechanism subjects the medial side to tension, leading potentially to rupture of the Deltoid ligament or an associated avulsion fracture of the **medial malleolus**. *Anterior talofibular ligament*- This is the **most commonly injured** ligament in the ankle, typically resulting from an **inversion injury** combined with plantar flexion.- It connects the fibula to the talus and is the weakest of the lateral ligaments, making it the primary target of **lateral ankle sprains**. *Calcaneofibular ligament*- This ligament also acts as a restraint against **inversion** and is located laterally, deep to the peroneal tendons.- Injury to the CFL often occurs when the foot is **dorsiflexed** and inverted, usually damaged secondarily after the **ATFL** tears. *Posterior talofibular ligament*- Located on the posterior-lateral aspect, this ligament is the **strongest** of the lateral stabilizers.- It is rarely injured in isolated ligamentous sprains, typically requiring severe **dislocations** or extensive high-grade **inversion injuries**.
About NEET-PG 2025 Questions
This page contains 175 questions from the NEET-PG 2025 paper, organised across 19 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the NEET-PG exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your NEET-PG goals.