Which of the following is not seen with ileal resections?
A nasal surgery was carried out with the incision shown in the image. What was the procedure likely carried out?

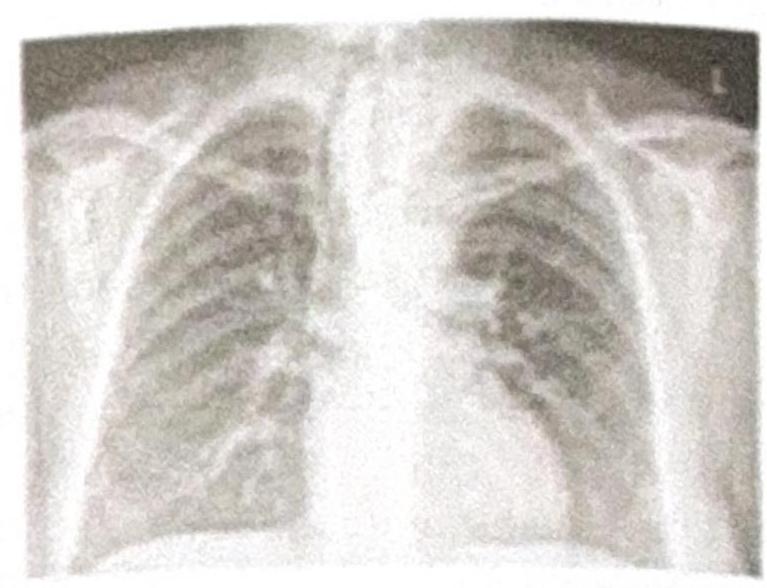
Which of the following procedures would be difficult to perform based on the given Chest X-ray?
A patient presents with an umbilical mass, which was previously reducible but has now become irreducible with discharge coming out, as shown in the image. What is the most appropriate management?

NEET-PG 2024 - Surgery NEET-PG Practice Questions and MCQs
Question 21: Which of the following is not seen with ileal resections?
- A. Microcytic hypochromic anemia
- B. Nuclear cytological asynchrony
- C. Neurological manifestation
- D. Cognitive improvement (Correct Answer)
Explanation: ***Cognitive improvement*** - Ileal resections are associated with malabsorption of various nutrients, but they do not lead to **cognitive improvement**. In fact, nutrient deficiencies (particularly B12) can negatively impact cognitive function. - The effects of ileal resections are primarily related to **digestion** and **absorption**, causing symptoms like diarrhea, weight loss, and specific vitamin deficiencies, not enhanced brain function. - This is the **most obvious answer** to what is "not seen" with ileal resections. *Microcytic hypochromic anemia* - This type of anemia is caused by **iron deficiency**, which is **NOT a direct consequence** of ileal resection. - **Iron absorption** occurs primarily in the **duodenum and proximal jejunum**, not in the ileum. - Ileal resection typically causes **macrocytic anemia** (due to B12 deficiency), not microcytic anemia. - While microcytic anemia could occur indirectly from chronic blood loss in inflammatory bowel disease, it is not a characteristic feature of ileal resection itself. *Nuclear cytological asynchrony* - **Nuclear cytological asynchrony** (megaloblastic changes) is a **direct consequence** of **vitamin B12 deficiency**, which commonly results from terminal ileal resection. - The **terminal ileum** is the primary site for absorption of **vitamin B12** (cobalamin) bound to intrinsic factor. - This manifests as macrocytic anemia with characteristic bone marrow changes. *Neurological manifestation* - **Vitamin B12 deficiency**, resulting from impaired absorption after ileal resection, directly causes various **neurological symptoms**. - These include **peripheral neuropathy**, **subacute combined degeneration of the spinal cord** (posterior and lateral columns), paresthesias, ataxia, memory impairment, and cognitive changes. - Neurological symptoms may occur even before hematological changes become apparent.
Question 22: A nasal surgery was carried out with the incision shown in the image. What was the procedure likely carried out?
- A. Submucosal resection (SMR)
- B. FESS (Functional Endoscopic Sinus Surgery)
- C. Open rhinoplasty (Correct Answer)
- D. Caldwell-Luc's procedure
Explanation: ***Open rhinoplasty*** - The image displays a **transcolumellar incision** (typically inverted V or W-shaped), which is the hallmark approach for **open rhinoplasty**. - This incision allows for direct visualization of the underlying nasal cartilages and bones, enabling precise reshaping of the nose. *Submucosal resection (SMR)* - SMR is a procedure to correct a **deviated nasal septum** by removing cartilage or bone from beneath the mucoperichondrial flaps. - It involves an **intranasal incision**, usually along the septal mucosa, not an external transcolumellar incision. *FESS (Functional Endoscopic Sinus Surgery)* - FESS is a minimally invasive procedure used to treat **chronic sinusitis** and other sinus conditions. - It is performed entirely **endoscopically through the nostrils**, with no external incisions on the nasal columella. *Caldwell-Luc's procedure* - This procedure accesses the **maxillary sinus** through an incision in the upper gum beneath the lip. - It is used for drainage of the maxillary sinus or removal of foreign bodies/tumors, and does not involve an external nasal incision.
Question 23: Which of the following procedures would be difficult to perform based on the given Chest X-ray?
- A. Tracheostomy (Correct Answer)
- B. Laryngeal mask airway insertion
- C. Ryle's tube insertion
- D. Intubation
Explanation: ***Tracheostomy*** - The chest X-ray shows the presence of a **large thyroid mass** (appearing as a soft tissue density in the neck and upper mediastinum), which would displace the trachea and obscure anatomical landmarks, making a tracheostomy technically challenging and increasing the risk of complications. - A tracheostomy requires clear access to the anterior tracheal wall, which would be **directly obstructed** by the prominent thyroid hypertrophy visible on the X-ray. - This makes tracheostomy the **most difficult** procedure among the options, with significant risk of bleeding from engorged thyroid vessels and difficulty identifying the trachea. *Laryngeal mask airway insertion* - Laryngeal mask airway (LMA) insertion primarily involves placing a device over the **laryngeal inlet** and is not significantly affected by a mass lower in the neck impacting the trachea. - The LMA is a supraglottic device, and its placement does not require direct access to the trachea itself or the deeper structures of the neck. *Ryle's tube insertion* - Ryle's tube (nasogastric tube) insertion involves passing a tube from the **nose or mouth into the esophagus and stomach**. - This procedure is generally unaffected by a thyroid mass, as it primarily involves the gastrointestinal tract, which is anatomically separate from the trachea in the neck region. *Intubation* - Intubation (endotracheal intubation) involves placing a tube into the **trachea via the mouth or nose**, usually past the vocal cords. - While a large retrosternal thyroid mass can cause tracheal deviation and compression that may complicate intubation, it is generally **less difficult than tracheostomy** in this scenario. - Intubation can often be achieved with experienced anesthesia techniques (videolaryngoscopy, fiberoptic intubation), whereas tracheostomy faces direct surgical field obstruction by the thyroid mass itself. - The primary challenge for intubation is visualization and navigation past the vocal cords, not the direct anatomical obstruction at the surgical site that makes tracheostomy particularly difficult.
Question 24: A patient presents with an umbilical mass, which was previously reducible but has now become irreducible with discharge coming out, as shown in the image. What is the most appropriate management?
- A. Umbilical excision
- B. Umbilical excision with mesh hernioplasty (Correct Answer)
- C. Mesh hernioplasty
- D. Conservative
Explanation: ***Umbilical excision with mesh hernioplasty*** - The presence of an **irreducible umbilical mass with discharge** indicates a complicated umbilical hernia, likely with **incarceration, strangulation, or infection**. - Management requires **excision of compromised tissue** (umbilicus and surrounding necrotic/infected skin) followed by **hernia defect repair**. - **Mesh hernioplasty** provides strong, durable reinforcement and prevents recurrence. - **Note:** In heavily contaminated fields, primary tissue repair or biologic mesh may be preferred over synthetic mesh, or staged repair may be considered. However, if contamination is minimal after debridement, mesh repair can be performed in the same setting. *Umbilical excision* - While **excision of the compromised umbilical skin and necrotic tissue** is necessary due to the discharge (suggesting infection or necrosis), **excision alone does not address the underlying hernia defect**. - Simply excising the umbilicus without repairing the hernia would lead to **persistent hernia or recurrence**. *Mesh hernioplasty* - A mesh hernioplasty alone is appropriate for **uncomplicated, reducible umbilical hernias** to reinforce the abdominal wall. - However, it **does not account for the irreducibility and skin changes/discharge**, which necessitate **excision of potentially infected or necrotic tissue** first. - Placing mesh without addressing the compromised tissue would risk ongoing infection and mesh complications. *Conservative* - **Conservative management** is reserved for **asymptomatic, reducible umbilical hernias** in adults (especially if small) or for infants where spontaneous closure can occur. - An **irreducible mass with discharge** signifies an **acute surgical emergency** (incarceration, strangulation, or infection) requiring **urgent surgical intervention**, not observation.