All SubjectsAnatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q11
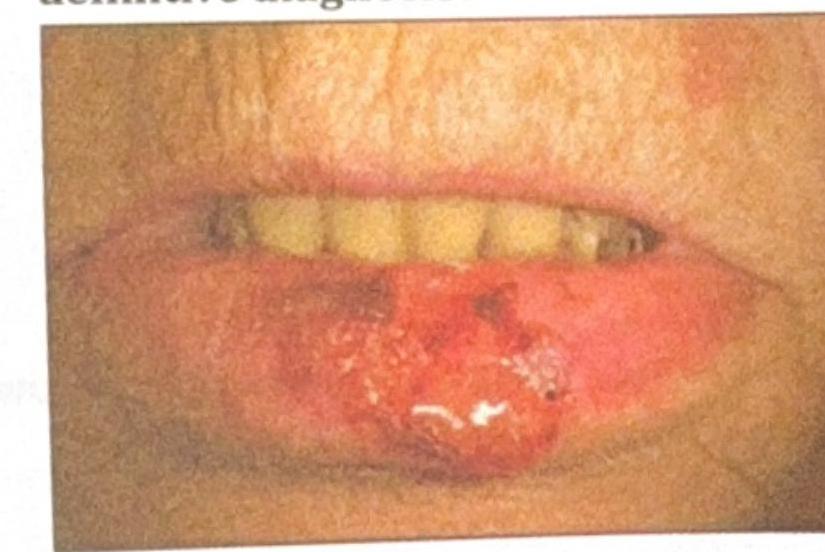
An elderly patient presents with a non-healing ulcerative lesion on the lower lip, as shown in the image. The lesion has been gradually enlarging over the past few months. Suspecting squamous cell carcinoma (SCC), what is the most appropriate method to obtain a biopsy for definitive diagnosis?
Q12
How does a skin graft receive nutrition on day 3 after transplantation?
Q13
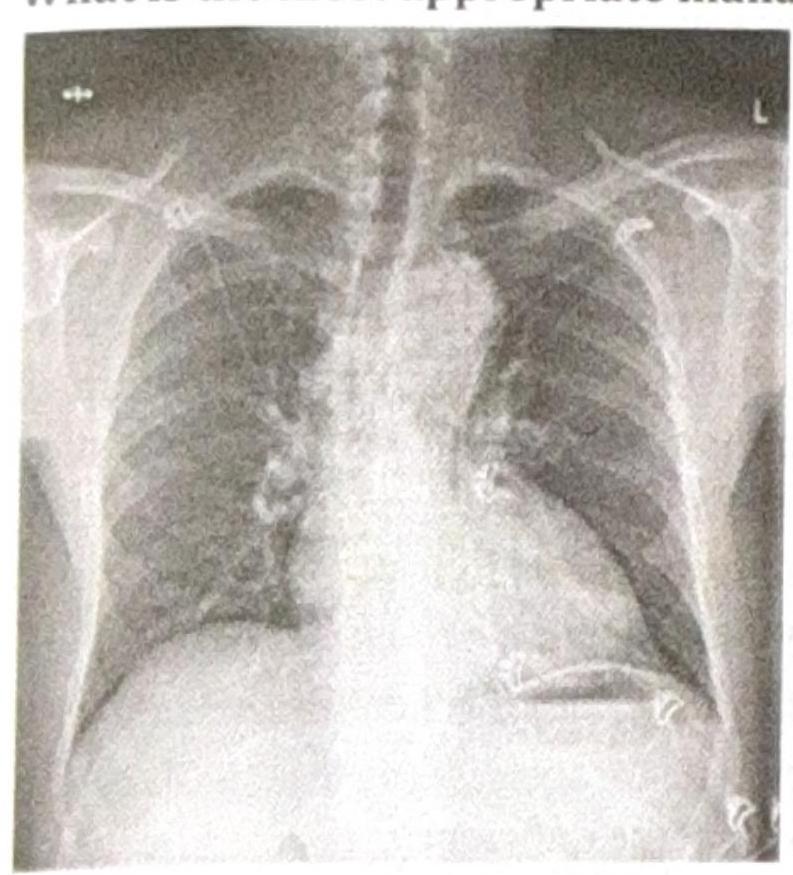
A patient presents with constant chest pain, and the radiological finding is as shown in the image. What is the most appropriate management?
Q14
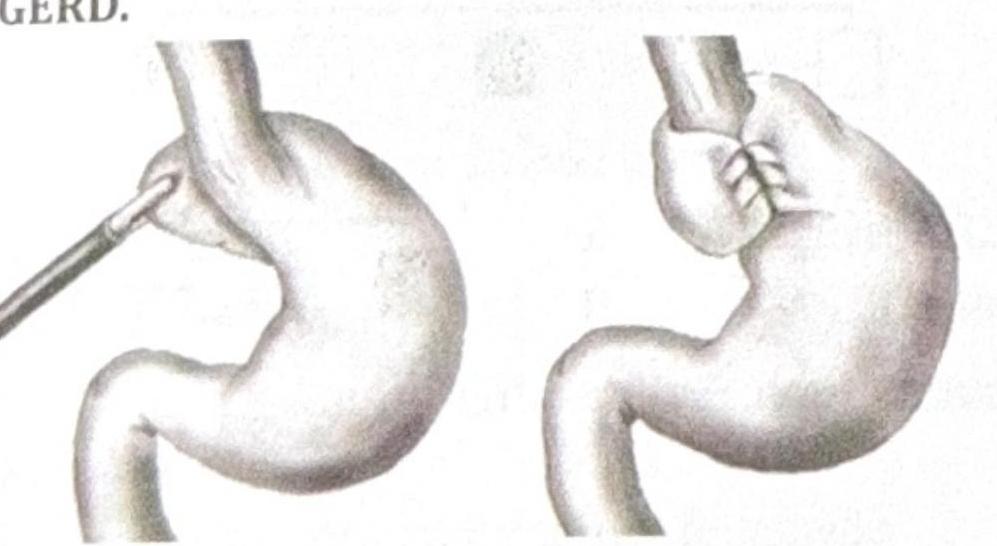
Identify the procedure shown in the image, which is performed in a patient with recurrent GERD.
Q15
A patient presents with a penile lesion staged as T3, with clinically palpable lymph nodes. What is the most appropriate management?
Q16
A patient presents with fecal discharge from the umbilicus. What is the most likely diagnosis?
Q17
What is the diagnosis based on the image shown?

Q18
Which of the following is not seen with ileal resections?
Q19
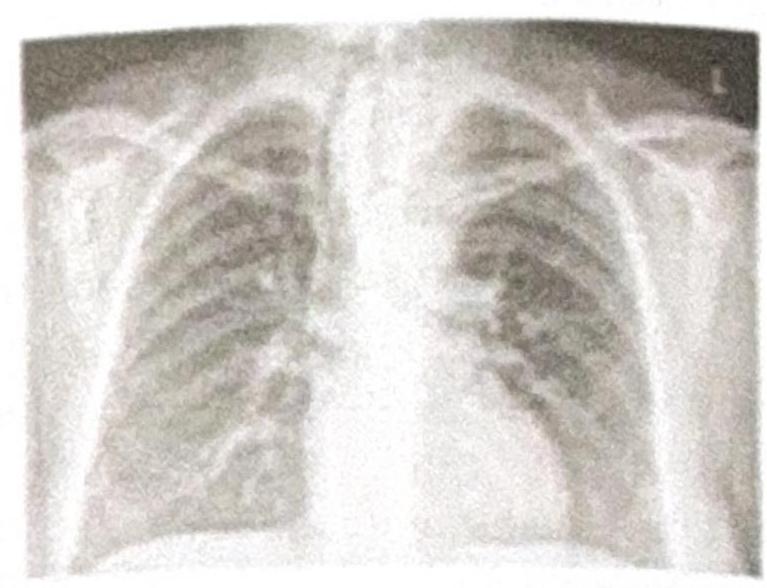
Which of the following procedures would be difficult to perform based on the given Chest X-ray?
Q20
A patient presents with an umbilical mass, which was previously reducible but has now become irreducible with discharge coming out, as shown in the image. What is the most appropriate management?
