NEET-PG 2024 — Surgery
24 Previous Year Questions with Answers & Explanations
Identify the instrument shown in the image:
A hypertensive patient presents with excruciating chest pain and unequal radial pulses. Which of the following is the correct management for this patient?
A 78-year-old immobile patient presents with a pressure ulcer on the sacral area, as shown in the image below. How would you grade this bedsore?
The image shows a Negative Pressure Wound Therapy (NPWT) dressing applied to a patient's wound. What is the ideal negative pressure range commonly used for NPWT to promote wound healing?

Which of these is the STRONGEST indication for giving adjuvant treatment in oral malignancy after resection and Modified Radical Neck Dissection (MRND)?
A patient presents to the OPD with a right-sided ulcerated breast lesion. Radiological imaging shows liver metastasis, as seen in the provided ultrasound image. What is the most appropriate management?

Identify the instrument shown in the image.
What type of graft or dressing is used to cover the post-burn wound shown in the image?
A jeep driver presents with pain in the gluteal region along with swelling and pus discharge for the past 6 months. What is the most likely diagnosis?
Surgery was performed as shown in the image below. What is the name of the procedure?
NEET-PG 2024 - Surgery NEET-PG Practice Questions and MCQs
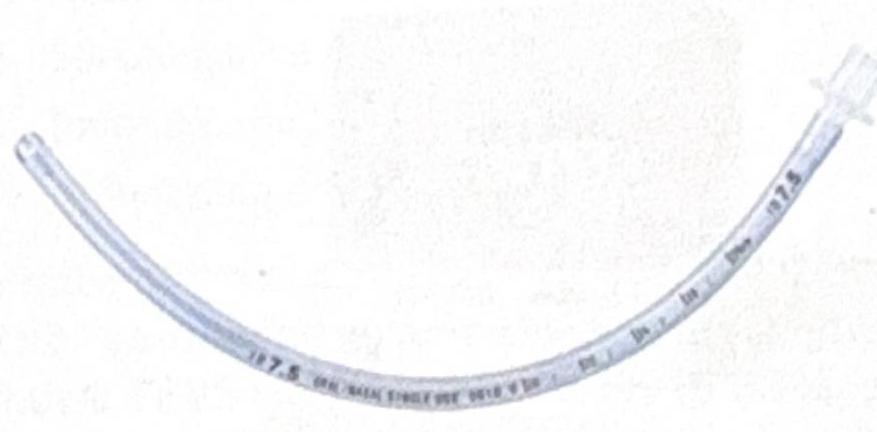
Question 1: Identify the instrument shown in the image:
- A. Nasogastric tube
- B. Uncuffed endotracheal (ET) tube (Correct Answer)
- C. Oropharyngeal tube
- D. Tracheostomy tube
Explanation: ***Uncuffed endotracheal (ET) tube*** - This image displays a transparent, flexible tube with a distinct connector at one end and no inflated cuff near the distal tip, which is characteristic of an **uncuffed endotracheal tube**. - Uncuffed ET tubes are commonly used in **pediatric patients** where a cuff could potentially damage the narrower, cone-shaped trachea. *Nasogastric tube* - A nasogastric tube typically has a much **smaller diameter** and a distinctly different tip design, often with multiple side ports for fluid aspiration or administration. - It does not feature the large, universal connector seen on endotracheal tubes. *Oropharyngeal tube* - An oropharyngeal (Guedel) airway is a **rigid, curved device** inserted into the mouth to maintain an open airway, and it looks distinctly different from the flexible tube shown. - It does not extend into the trachea like an ET tube. *Tracheostomy tube* - A tracheostomy tube is typically shorter, often with a curved neck flange for securement to the neck, and frequently made with an outer and inner cannula, which are absent in the image. - While it helps maintain an airway, its design is specific for insertion directly into a tracheostomy stoma, unlike the longer tube for oral/nasal intubation.
Question 2: A hypertensive patient presents with excruciating chest pain and unequal radial pulses. Which of the following is the correct management for this patient?
- A. Emergency surgical repair (Correct Answer)
- B. BP control and monitoring
- C. Stenting
- D. Balloon dilatation
Explanation: ***Emergency surgical repair*** - The combination of **excruciating chest pain**, a history of **hypertension**, and **unequal radial pulses** is highly suggestive of an **acute aortic dissection**. - **Unequal radial pulses** indicate involvement of the **ascending aorta** (Type A dissection), affecting the brachiocephalic or subclavian arteries that branch proximally from the aortic arch. - **Type A aortic dissections**, involving the ascending aorta, are life-threatening emergencies requiring immediate **surgical repair** to prevent rupture, cardiac tamponade, aortic regurgitation, and organ malperfusion. *BP control and monitoring* - While **blood pressure control** is a crucial initial step in managing aortic dissection to reduce shear stress on the aorta and prevent propagation, it is insufficient as the primary treatment for an **ascending (Type A) aortic dissection**. - Continuous monitoring is necessary but cannot resolve a progressing dissection that poses an immediate threat to life. - Medical management alone is reserved for **uncomplicated Type B dissections**. *Stenting* - **Endovascular stenting** (thoracic endovascular aortic repair, TEVAR) is primarily used for **Type B aortic dissections** (involving the descending aorta) in stable patients or those with complicated features. - It is generally not the first-line treatment for **Type A dissections** due to the anatomical challenges and urgent need for surgical repair in this location. *Balloon dilatation* - **Balloon dilatation** or angioplasty is a procedure used to open narrowed arteries, typically in the context of atherosclerotic disease (e.g., coronary artery disease or peripheral artery disease). - It has no role in the management of an **aortic dissection**, which involves a tear in the aortic wall rather than a simple narrowing.
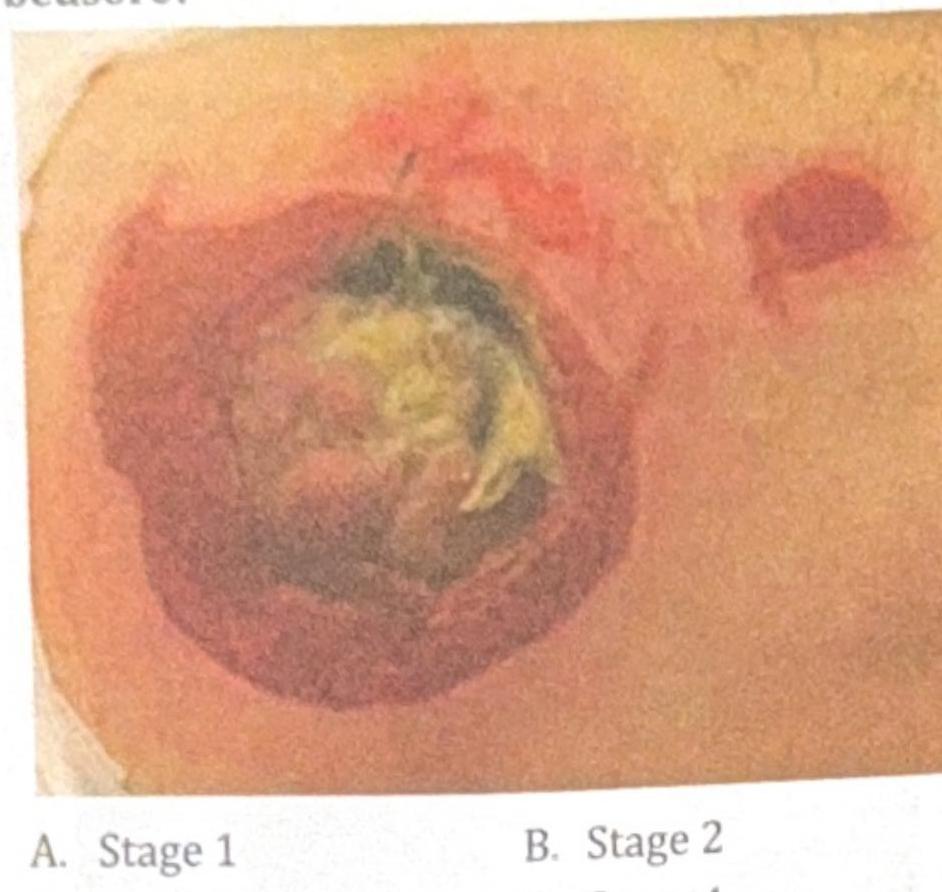
Question 3: A 78-year-old immobile patient presents with a pressure ulcer on the sacral area, as shown in the image below. How would you grade this bedsore?
- A. Stage 1
- B. Stage 2
- C. Stage 3
- D. Stage 4 (Correct Answer)
Explanation: *Stage 1* - A Stage 1 pressure ulcer is characterized by **non-blanchable erythema** of intact skin, typically over a bony prominence. - There is no break in the skin, which is not what is visible in the image. *Stage 2* - A Stage 2 pressure ulcer involves **partial-thickness skin loss** presenting as a shallow open ulcer with a red-pink wound bed, without slough or bruising. - The depth and tissue involvement shown in the image are far more extensive than a Stage 2 ulcer. *Stage 3* - A Stage 3 pressure ulcer involves **full-thickness tissue loss** where subcutaneous fat may be visible, but bone, tendon, or muscle are not exposed. - The visible structures in the image suggest involvement beyond the subcutaneous fat layer, distinguishing it from a Stage 3 ulcer. ***Stage 4*** - The image shows **full-thickness tissue loss** with visible **bone, tendon, or muscle**, indicating a Stage 4 pressure ulcer. - There is also evidence of **slough and eschar** in the wound bed, which is consistent with severe tissue damage extending beyond the subcutaneous fat. - This is the **correct answer** as the exposed deeper structures are pathognomonic for Stage 4.
Question 4: The image shows a Negative Pressure Wound Therapy (NPWT) dressing applied to a patient's wound. What is the ideal negative pressure range commonly used for NPWT to promote wound healing?
- A. -125 mm Hg (Correct Answer)
- B. 60-80 mm Hg
- C. 130 mm Hg
- D. 80-100 mm Hg
Explanation: ***-125 mm Hg*** - **Negative Pressure Wound Therapy (NPWT)** uses controlled subatmospheric (negative) pressure to promote wound healing. - The most commonly used pressure setting is **-125 mm Hg**, which has been extensively validated in clinical studies. - This pressure level effectively promotes granulation tissue formation, reduces edema, removes exudate, and increases blood flow to the wound bed. - **-75 to -125 mm Hg** is the typical therapeutic range, with -125 mm Hg being the standard setting for most wound types. *60-80 mm Hg* - This represents **positive pressure**, not negative pressure used in NPWT. - NPWT requires subatmospheric (below atmospheric) pressure, denoted by the negative sign. - Positive pressures in this range would be used in compression therapy for venous insufficiency, not vacuum-assisted wound closure. *130 mm Hg* - This is a **positive pressure** value and does not apply to NPWT. - NPWT uses negative (suction) pressure, not positive compression. - If interpreted as -130 mm Hg, this would be at the higher end and might increase patient discomfort without additional benefit over -125 mm Hg. *80-100 mm Hg* - These are **positive pressure** values not used in NPWT. - NPWT specifically requires negative pressure (vacuum/suction) to work effectively. - This range would be excessively high even for compression therapy and inappropriate for NPWT.
Question 5: Which of these is the STRONGEST indication for giving adjuvant treatment in oral malignancy after resection and Modified Radical Neck Dissection (MRND)?
- A. Extranodal extension (Correct Answer)
- B. Multiple lymph node metastasis
- C. T3 tumor
- D. Close margin
Explanation: ***Extranodal extension*** - **Extranodal extension (ENE)** is the strongest adverse pathological feature (APF) indicating the highest risk of recurrence and significantly impacting prognosis. - ENE is associated with increased likelihood of regional and distant metastasis. - The presence of ENE mandates **adjuvant concurrent chemoradiotherapy** (not radiotherapy alone), as landmark trials (EORTC 22931, RTOG 9501) demonstrated survival benefit with combined modality treatment. - ENE and positive surgical margins are the two most critical features requiring intensified adjuvant therapy. *Multiple lymph node metastasis* - Multiple positive lymph nodes (≥2 nodes) indicate high risk of recurrence and warrant **adjuvant radiotherapy**. - While this is a significant adverse feature, it does not mandate chemoradiotherapy unless accompanied by ENE or positive margins. - Considered a high-risk feature but not as strong an indication as ENE. *T3 tumor* - T3 tumor indicates significant local invasion but is a clinical staging parameter, not a pathological adverse feature. - The decision for adjuvant therapy depends primarily on pathological findings (margins, lymph node status, ENE) rather than T-stage alone. - T3 status without adverse pathological features may not require adjuvant treatment after complete resection. *Close margin* - Close margin (tumor within 1-5 mm of resected edge) is a high-risk feature warranting **adjuvant radiotherapy** due to increased local recurrence risk. - However, it is less critical than ENE in terms of overall survival and regional control. - A **positive margin** (<1 mm or tumor at ink) would be equivalent to ENE as an indication for chemoradiotherapy, but a close margin typically requires radiotherapy alone.
Question 6: A patient presents to the OPD with a right-sided ulcerated breast lesion. Radiological imaging shows liver metastasis, as seen in the provided ultrasound image. What is the most appropriate management?
- A. Simple mastectomy
- B. Modified Radical Mastectomy (MRM)
- C. Radical mastectomy
- D. Neoadjuvant chemotherapy followed by surgery (Correct Answer)
Explanation: ***Neoadjuvant chemotherapy followed by surgery*** - The presence of **distant metastasis** (liver metastasis) indicates **Stage IV breast cancer**, where **systemic treatment is the primary goal**. - In Stage IV disease, **palliative systemic chemotherapy** is the mainstay of treatment to control distant disease and improve survival. - Surgery in metastatic breast cancer may be considered for **local control of symptomatic disease** (ulceration, bleeding, pain), typically after initiating systemic therapy. - The combination of systemic therapy followed by local surgery for the ulcerated lesion addresses both the metastatic disease and provides local symptom relief. *Simple mastectomy* - While this could provide local control of the ulcerated lesion, it does **not address the distant metastasis**. - In Stage IV disease, **systemic therapy must be prioritized** before considering any local surgical intervention. - Surgery alone without systemic treatment would be inadequate for metastatic disease. *Modified Radical Mastectomy (MRM)* - MRM involves removal of the entire breast tissue, skin, nipple-areolar complex, and level I and II axillary lymph nodes. - While this provides comprehensive local-regional control, it **does not address distant metastasis**. - In Stage IV disease, extensive locoregional surgery without systemic therapy first would be inappropriate, as the primary issue is systemic disease. *Radical mastectomy* - This extensive procedure involves removal of the breast, axillary lymph nodes, and pectoralis muscles. - It is **rarely performed today** due to significant morbidity and no survival benefit over less extensive procedures. - Like other surgical options alone, it fails to address the systemic nature of Stage IV disease.
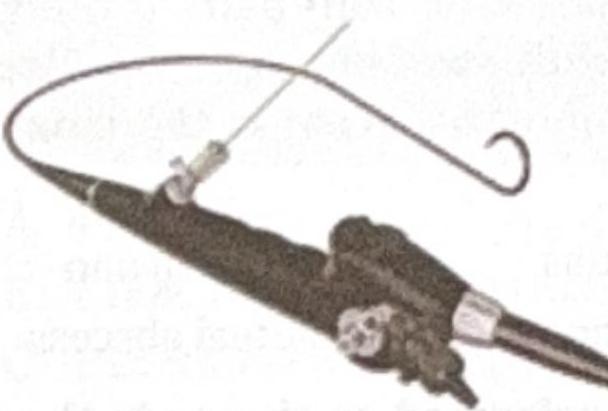
Question 7: Identify the instrument shown in the image.
- A. Nephroscope
- B. Cystoscope
- C. Ureteroscope (Correct Answer)
- D. Laparoscope
Explanation: ***Ureteroscope*** - The image distinctly shows a long, thin, flexible scope with a working channel, consistent with a **flexible ureteroscope**. - The presence of a **guidewire** alongside the scope further indicates its use for navigating the narrow and tortuous ureter. *Nephroscope* - A nephroscope is typically a more rigid and wider instrument used for percutaneous access to the **kidney's collecting system**. - Its design is optimized for procedures within the kidney, not for navigating the ureter. *Cystoscope* - A cystoscope is used to visualize the **bladder** and urethra and is generally shorter and thicker than a ureteroscope. - While it can be flexible or rigid, the instrument shown is too long and thin to be a standard cystoscope. *Laparoscope* - A laparoscope is a rigid instrument used for **abdominal surgery**, inserted through the abdominal wall. - Its design and application are entirely different from the instrument shown, which is designed for internal urinary tract procedures.
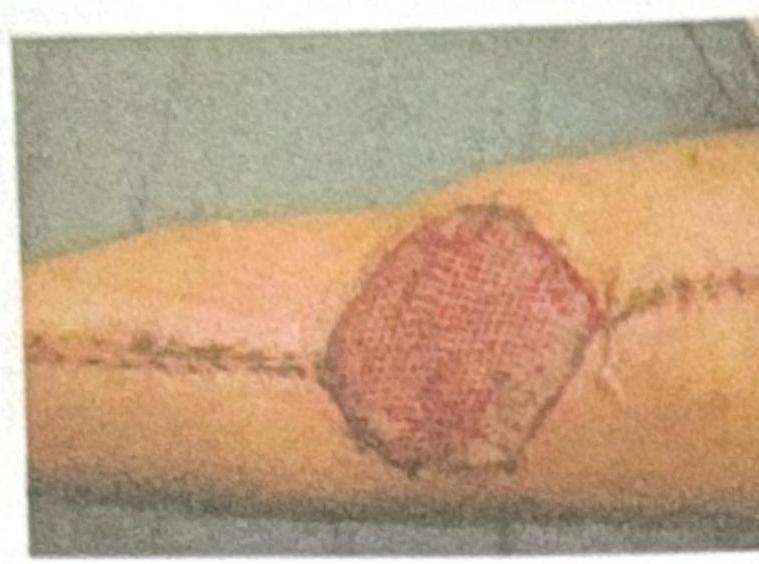
Question 8: What type of graft or dressing is used to cover the post-burn wound shown in the image?
- A. Split thickness skin graft (Correct Answer)
- B. Full thickness skin graft
- C. VAC dressing
- D. Normal saline dressing
Explanation: ***Split thickness skin graft*** - The image shows a **meshed pattern** on the skin graft, which is characteristic of a **split-thickness skin graft** that has been expanded to cover a larger area. - This type of graft consists of the epidermis and a portion of the dermis, making it more flexible and able to **"take" more reliably** on various wound beds, commonly used for burn wounds. *Full thickness skin graft* - A **full-thickness skin graft** includes the entire epidermis and dermis and typically does not have a meshed appearance. - They are used for smaller defects where cosmesis is a priority, but have a **lower take rate** than split-thickness grafts, making them less suitable for large burn wounds. *VAC dressing* - A **VAC (Vacuum-Assisted Closure) dressing** is a system that applies negative pressure to a wound to promote healing and is not a skin graft itself. - It involves a foam or gauze dressing sealed with an adhesive film, connected to a vacuum pump, which is not what is depicted in the image. *Normal saline dressing* - A **normal saline dressing** is a simple wet-to-dry or wet-to-wet dressing for wound care, involving gauze soaked in normal saline. - This is a basic wound management technique and does not involve grafting or have the characteristic meshed appearance seen in the image.
Question 9: A jeep driver presents with pain in the gluteal region along with swelling and pus discharge for the past 6 months. What is the most likely diagnosis?
- A. Fistula in ano
- B. Fissure in ano
- C. Gluteal abscess
- D. Pilonidal sinus (Correct Answer)
Explanation: ***Pilonidal sinus*** - This is the classic presentation of **pilonidal sinus disease**, historically known as **"Jeep disease"** due to its high incidence in military personnel during WWII who sat for prolonged periods in jeeps - The **occupational clue "jeep driver"** is pathognomonic for pilonidal sinus, as prolonged sitting causes friction and pressure in the **sacrococcygeal/natal cleft region** - Presents with **chronic pain, swelling, and intermittent pus discharge** in the gluteal region, typically over weeks to months - Risk factors include: prolonged sitting, friction, deep natal cleft, obesity, and excessive body hair - The **chronic 6-month duration** with ongoing discharge is characteristic of pilonidal sinus with secondary infection, not an acute abscess *Gluteal abscess* - While this can cause pain, swelling, and pus discharge, it typically presents **acutely** (days to weeks, not 6 months) - Does not have the specific **occupational association with prolonged sitting** (jeep driver) - Would be expected to either resolve with drainage/antibiotics or progress to sepsis, not persist chronically for 6 months - Lacks the classic "Jeep disease" eponym *Fistula in ano* - This involves an abnormal tract between the **anal canal and perianal skin** - Discharge would be localized **perianally**, close to the anus, not in the broader gluteal/sacrococcygeal region - Does not have the jeep driver occupational association *Fissure in ano* - A **tear in the anal canal lining** causing severe pain during defecation with **bright red bleeding** - Does not present with swelling or chronic pus discharge - Pain is characteristically related to bowel movements, not constant
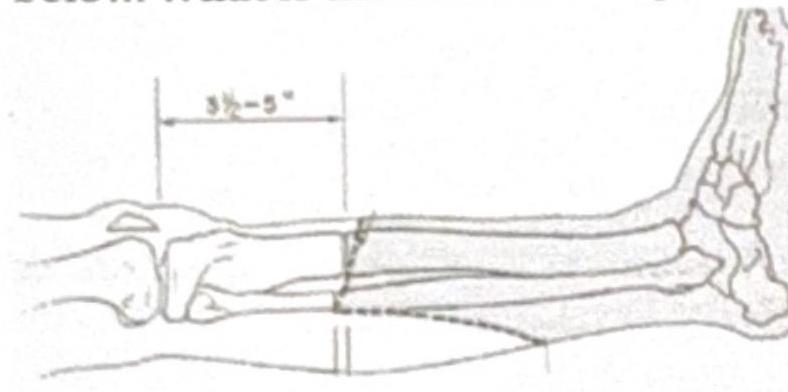
Question 10: Surgery was performed as shown in the image below. What is the name of the procedure?
- A. Below knee amputation
- B. Above knee amputation
- C. Lisfranc amputation
- D. Chopart amputation (Correct Answer)
Explanation: ***Chopart amputation*** - The image shows a disarticulation through the **talonavicular and calcaneocuboid joints**, which defines a **Chopart amputation**. - This procedure removes the distal foot while preserving the **calcaneus and talus**, forming a stump that allows for some ankle motion. *Below knee amputation* - A below-knee amputation involves transection of the tibia and fibula, preserving the knee joint, which is much more proximal than shown in the image. - This type of amputation removes a significant portion of the lower leg, with the foot entirely removed, unlike the partial foot amputation depicted. *Above knee amputation* - An above-knee amputation involves disarticulation or transection through the femur, completely removing the lower leg and knee joint. - This is a much more extensive amputation than what is illustrated, which is confined to the foot. *Lisfranc amputation* - A Lisfranc amputation is a disarticulation through the **tarsometatarsal joints**, removing the metatarsals and phalanges but preserving the tarsal bones. - The image clearly shows the incision more proximally, at the midtarsal level, specifically through the talonavicular and calcaneocuboid joints, not the tarsometatarsal joints.