NEET-PG 2024 — Radiology
14 Previous Year Questions with Answers & Explanations
Identify the investigation being carried out in the image.
What condition does the MRCP (Magnetic Resonance Cholangiopancreatography) image indicate?

A patient presents with foul-smelling sputum along with breathlessness and fever. Using the X-ray below, identify the diagnosis.
What is the Diagnosis based on the CT Scan given below?
A 25-year-old male presents with chest pain and shortness of breath. A CT scan of the chest is performed, and the image provided shows a large, well-defined mass in the anterior mediastinum. The mass contains both cystic and solid components, along with areas of calcification. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?
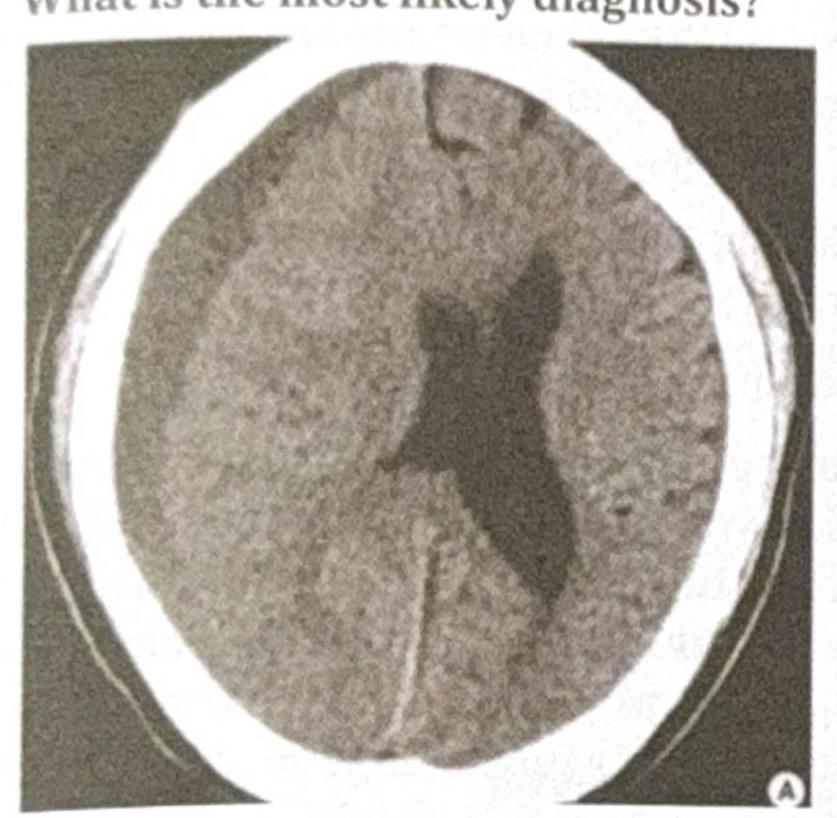
An 80-year-old male with a history of frequent falls presents with progressive headache, confusion, and mild hemiparesis over the past few weeks. A CT scan of the head is performed, and the image provided shows a crescent-shaped, hypodense collection over the left cerebral hemisphere with a slight midline shift. What is the most likely diagnosis?
A 40-year-old male presents with a history of headaches, fever, and new-onset seizures. An MRI of the brain is performed, revealing a ring-enhancing lesion with central restricted diffusion on diffusion-weighted imaging (DWI). What is the most likely diagnosis?
A 45-year-old farmer presents with right upper quadrant pain and a history of exposure to livestock. An abdominal ultrasound shows a cystic lesion in the liver with internal floating membranes, described as the "Water lily sign." Based on this finding, what is the most likely Gharbi classification stage of the hydatid cyst?

A man presents with back pain following a road traffic accident (RTA). There is no history of neurological deficit. An X-ray of the spine is done. What is the diagnosis based on the image?

Identify the condition shown in the given X-ray:

NEET-PG 2024 - Radiology NEET-PG Practice Questions and MCQs
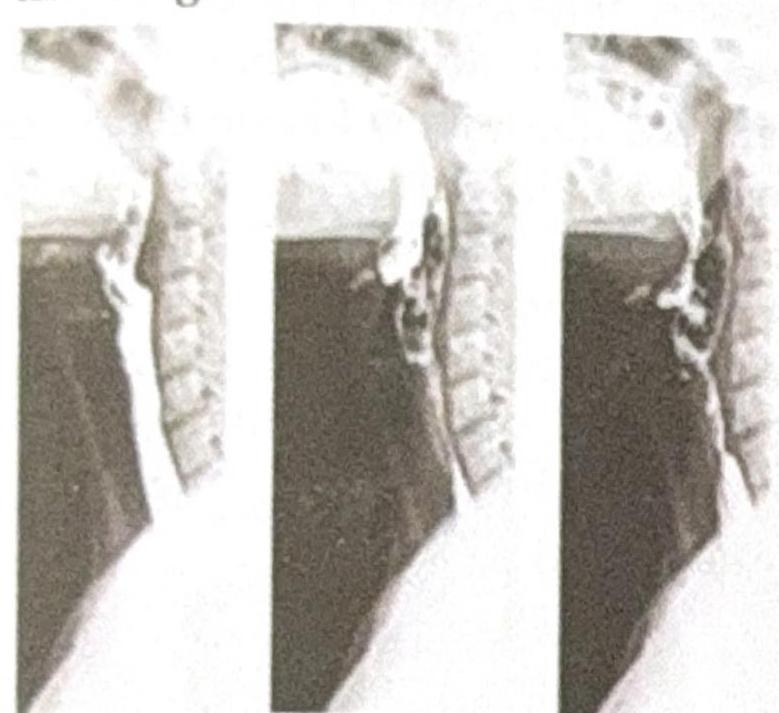
Question 1: Identify the investigation being carried out in the image.
- A. Fluoroscopy
- B. X-ray after alkali ingestion
- C. X-ray after acid ingestion
- D. Barium Swallow (Correct Answer)
Explanation: ***Barium Swallow*** - The image shows a contrast material, characteristic of **barium**, flowing through the esophagus, captured as a sequence of X-ray images, which is the definition of a barium swallow study. - This **dynamic imaging** allows for evaluation of swallowing function and esophageal motility. *Fluoroscopy* - While a barium swallow uses **fluoroscopy** to visualize the movement of barium, fluoroscopy itself is the technique, not the specific investigation being performed. The image depicts the result of a specific type of fluoroscopic examination. - Fluoroscopy is a general term for real-time X-ray imaging, whereas "Barium Swallow" specifies the type of study being done on the upper GI tract. *X-ray after alkali ingestion* - This scenario would typically involve viewing the effects of **corrosive injury** to the esophagus, which would appear as mucosal damage, narrowing, or perforation. The image does not show these features; instead, it shows smooth passage of contrast. - There is no visible evidence of an acute or chronic injury pattern consistent with **alkali ingestion**, which often leads to severe burns or strictures. *X-ray after acid ingestion* - Similar to alkali ingestion, acid ingestion also causes **corrosive injury**, typically affecting the stomach more severely than the esophagus. The image does not demonstrate these pathological changes. - The smooth, unobstructed flow of contrast in multiple frames is indicative of normal esophageal function rather than the sequelae of corrosive ingestion.
Question 2: What condition does the MRCP (Magnetic Resonance Cholangiopancreatography) image indicate?
- A. Choledochal cyst (Correct Answer)
- B. Dilated CBD (Common Bile Duct)
- C. Acute cholecystitis
- D. Cholangiocarcinoma
Explanation: **Choledochal cyst** - The MRCP image clearly shows a **cystic dilation** of the common bile duct, which is characteristic of a choledochal cyst. - This congenital anomaly involves saccular or fusiform dilation of the bile ducts, as depicted by the **balloon-like structure** in the image. - MRCP is the **gold standard imaging modality** for diagnosing choledochal cysts, providing excellent visualization of the biliary tree anatomy. *Dilated CBD (Common Bile Duct)* - While a choledochal cyst is a type of CBD dilation, simply stating "dilated CBD" is not specific enough, as the image shows a distinct **cystic morphology** beyond just uniform dilation. - Common bile duct dilation can be caused by various factors like stones or strictures, but the **focal, bulbous appearance** points specifically to a cyst. *Acute cholecystitis* - Acute cholecystitis typically presents with signs of gallbladder inflammation, such as **gallbladder wall thickening**, pericholecystic fluid, and gallstones, which are not depicted in this MRCP. - MRCP primarily visualizes the bile ducts and does not typically show the inflammatory changes of the gallbladder wall as clearly as ultrasound or CT. *Cholangiocarcinoma* - Cholangiocarcinoma usually manifests as a **stricture** or **mass** within the bile ducts, causing upstream dilation, rather than the isolated cystic dilation seen in the image. - There is no evidence of an obstructing mass or irregular narrowing within the bile ducts that would suggest a malignancy.
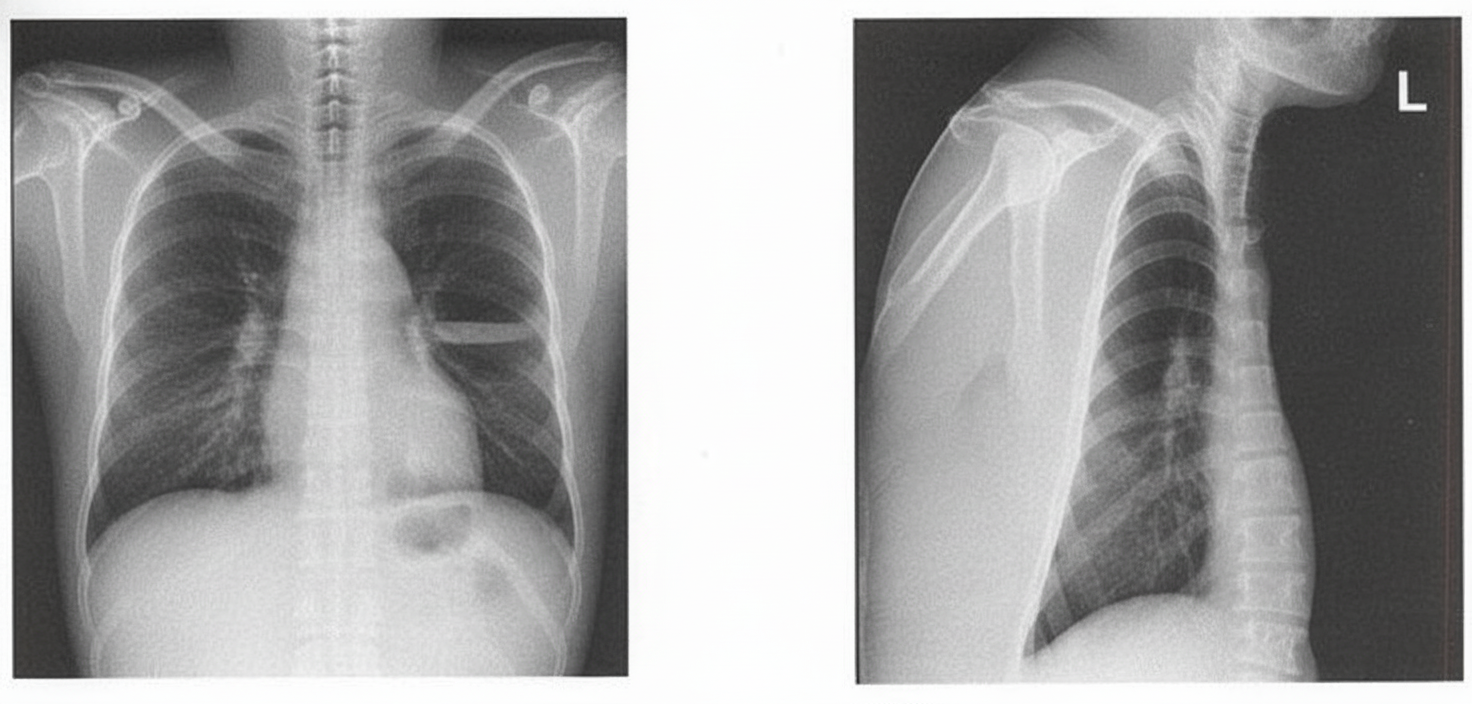
Question 3: A patient presents with foul-smelling sputum along with breathlessness and fever. Using the X-ray below, identify the diagnosis.
- A. Pneumothorax
- B. Pericardial Effusion
- C. Pleural Effusion
- D. Lung Abscess (Correct Answer)
Explanation: ***Lung Abscess*** - The combination of **foul-smelling sputum** (indicating anaerobic bacterial infection), breathlessness, and fever is **pathognomonic for lung abscess** - The X-ray demonstrates a **characteristic air-fluid level** within the lung parenchyma, which is the hallmark radiographic finding of a cavitating lung abscess - When a lung abscess ruptures into a bronchus, it produces the typical **foul-smelling, purulent sputum** described in this case - Common causes include aspiration pneumonia, particularly in patients with risk factors like alcoholism, poor dental hygiene, or altered consciousness *Pleural Effusion* - While pleural effusion can present with breathlessness and fever, it would **not produce foul-smelling sputum** - A simple pleural effusion appears as **blunting of the costophrenic angle** or a **meniscus sign**, not an air-fluid level within the lung field - An empyema (infected pleural effusion) with bronchopleural fistula could theoretically show an air-fluid level, but this would be in the **pleural space**, not within the lung parenchyma, and is much less common than lung abscess *Pneumothorax* - Pneumothorax shows **air in the pleural space** with visible lung edge and absent lung markings peripherally - There would be **no fluid component** and no foul-smelling sputum - The air-fluid level seen here indicates a cavitary lesion, not a pneumothorax *Pericardial Effusion* - Pericardial effusion presents with an **enlarged, globular cardiac silhouette** ("water bottle heart") - It would **not cause respiratory symptoms** like foul-smelling sputum or the radiographic findings shown - The pathology is clearly in the **lung field**, not around the heart
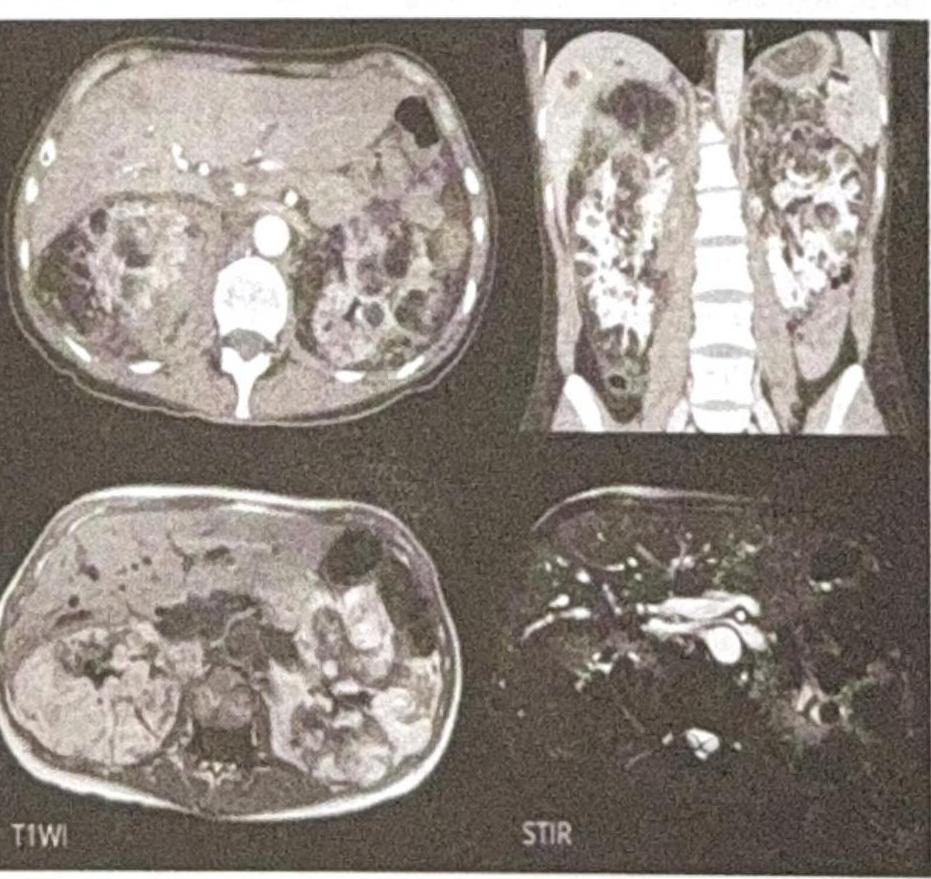
Question 4: What is the Diagnosis based on the CT Scan given below?
- A. Renal cyst
- B. Renal tumor
- C. Renal polycystic kidney disease (Correct Answer)
- D. Renal angiomyolipoma
Explanation: ***Polycystic kidney disease*** - The CT scan images show **enlarged kidneys** replaced by numerous **cysts of varying sizes**, which is the hallmark appearance of polycystic kidney disease. - The presence of multiple cysts **bilaterally** and diffusely throughout the renal parenchyma is characteristic of this genetic disorder. *Renal cyst* - A single renal cyst is a common benign finding, appearing as a **well-defined, fluid-filled** structure. - The images clearly demonstrate **multiple cysts** affecting both kidneys, ruling out a solitary renal cyst. *Renal tumor* - A renal tumor (e.g., renal cell carcinoma) typically appears as a **solid mass**, often with heterogeneous enhancement after contrast. - The lesions seen in the image are predominantly **cystic** and multifocal, which is inconsistent with a typical renal tumor. *Renal angiomyolipoma* - Renal angiomyolipomas are benign tumors containing **fat, smooth muscle, and blood vessels**, and they characteristically show **macroscopic fat** on CT scans. - While they can be multiple, especially in tuberous sclerosis, the dominant feature in the image is widespread cystic transformation, not fat-containing solid masses.
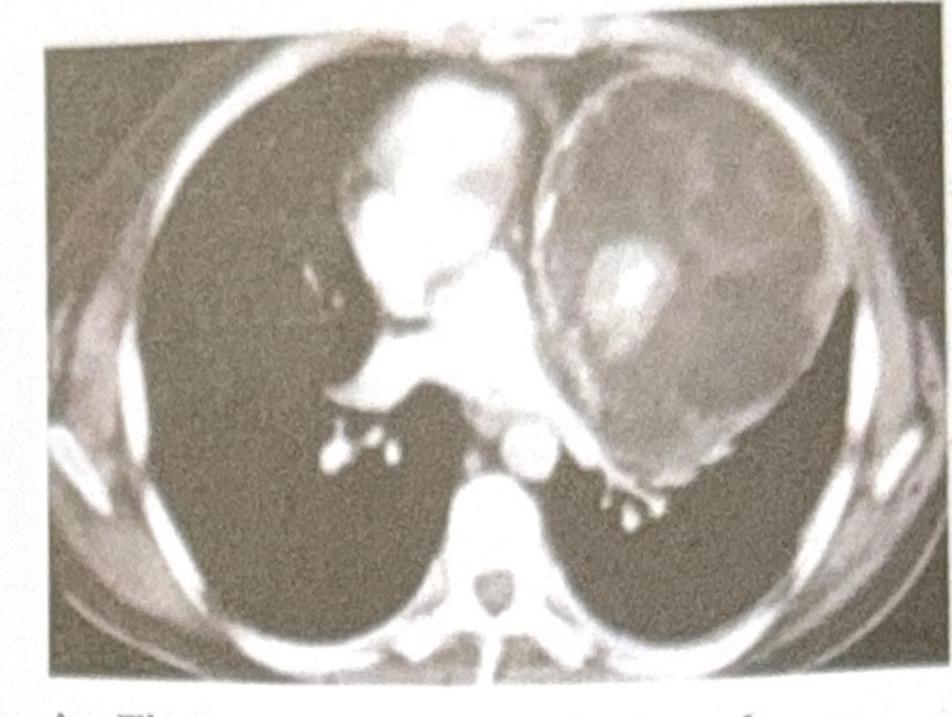
Question 5: A 25-year-old male presents with chest pain and shortness of breath. A CT scan of the chest is performed, and the image provided shows a large, well-defined mass in the anterior mediastinum. The mass contains both cystic and solid components, along with areas of calcification. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?
- A. Thymoma
- B. Lymphoma
- C. Teratoma (Correct Answer)
- D. Bronchogenic cyst
Explanation: ***Teratoma*** - The presence of a **well-defined anterior mediastinal mass** with **cystic and solid components** and **calcifications** is highly characteristic of a teratoma. - Teratomas are **germ cell tumors** containing tissues derived from all three embryonic germ layers, which explains their varied composition on imaging. *Thymoma* - While thymomas are common in the **anterior mediastinum**, they typically present as **solid masses** and calcifications are less common. - They are often associated with paraneoplastic syndromes like **myasthenia gravis**, which is not mentioned in this case. *Lymphoma* - Lymphoma in the anterior mediastinum often presents as a **lobulated, homogeneous mass**, and can be associated with **lymphadenopathy** elsewhere. - While it can be large, the specific features of cystic components and calcification are less typical for lymphoma. *Bronchogenic cyst* - Bronchogenic cysts are typically **unilocular, fluid-filled cystic lesions** and are usually found in the middle mediastinum or adjacent to the trachea/main bronchi. - They rarely contain significant solid components or calcifications, unlike the described mass.
Question 6: An 80-year-old male with a history of frequent falls presents with progressive headache, confusion, and mild hemiparesis over the past few weeks. A CT scan of the head is performed, and the image provided shows a crescent-shaped, hypodense collection over the left cerebral hemisphere with a slight midline shift. What is the most likely diagnosis?
- A. Acute subdural hematoma
- B. Epidural hematoma
- C. Chronic subdural hematoma (Correct Answer)
- D. Intracerebral hemorrhage
Explanation: ***Chronic subdural hematoma*** - The presented CT scan shows a **crescent-shaped, hypodense collection** over the left cerebral hemisphere, which is characteristic of a chronic subdural hematoma. **Hypodensity** indicates older, liquefied blood. - The patient's age (**80-year-old** with **frequent falls**), and the **progressive symptoms** (headache, confusion, mild hemiparesis over weeks) are highly consistent with a chronic rather than acute presentation. *Acute subdural hematoma* - An acute subdural hematoma would typically present as a **hyperdense** (bright) crescent-shaped collection on CT due to fresh blood. - Symptoms would usually be more acute and severe, developing over hours to days, which does not match the "past few weeks" progression. *Epidural hematoma* - An epidural hematoma is typically **lens-shaped (biconvex)**, not crescent-shaped, and usually results from a traumatic arterial bleed. - While it can cause midline shift, its characteristic shape and often acute presentation (often with a lucid interval) differentiate it from the described scenario. *Intracerebral hemorrhage* - An intracerebral hemorrhage occurs within the brain parenchyma, appearing as a **hyperdense mass within the brain tissue** on CT, not as a collection over the cerebral hemisphere. - The symptoms would depend on the location but would not typically involve a crescent-shaped collection outside the brain parenchyma.
Question 7: A 40-year-old male presents with a history of headaches, fever, and new-onset seizures. An MRI of the brain is performed, revealing a ring-enhancing lesion with central restricted diffusion on diffusion-weighted imaging (DWI). What is the most likely diagnosis?
- A. Glioblastoma multiforme
- B. Metastatic brain tumor
- C. Brain abscess (Correct Answer)
- D. Toxoplasmosis
Explanation: ***Brain abscess*** - A **ring-enhancing lesion** with **central restricted diffusion** on DWI is highly characteristic of a brain abscess, due to the presence of pus containing densely packed inflammatory cells and bacteria with high viscosity. - The clinical presentation of **headaches, fever**, and **new-onset seizures** is consistent with an infectious process and increased intracranial pressure. - This combination of imaging and clinical features is pathognomonic for pyogenic brain abscess. *Glioblastoma multiforme* - While GBM can present with **ring-enhancing lesions** and seizures, it typically exhibits **facilitated diffusion** (high ADC values) on DWI due to necrotic tumor core, not restricted diffusion. - GBM is a highly infiltrative tumor with extensive **vasogenic edema**. - Fever is uncommon in GBM unless there is secondary infection. *Metastatic brain tumor* - Metastatic lesions can be **ring-enhancing** and cause seizures, but **restricted diffusion** is not typical unless there is acute hemorrhage or superimposed infection. - The presence of **fever** points away from uncomplicated metastasis. - Multiple lesions at the gray-white matter junction are more typical of metastases. *Toxoplasmosis* - Toxoplasmosis in **immunocompromised individuals** (HIV/AIDS with CD4 <100) causes **multiple ring-enhancing lesions** with predilection for basal ganglia. - Restricted diffusion is **not consistently seen** with toxoplasmosis, unlike pyogenic abscesses. - The specific DWI finding of central restricted diffusion makes brain abscess the most definitive diagnosis.
Question 8: A 45-year-old farmer presents with right upper quadrant pain and a history of exposure to livestock. An abdominal ultrasound shows a cystic lesion in the liver with internal floating membranes, described as the "Water lily sign." Based on this finding, what is the most likely Gharbi classification stage of the hydatid cyst?
- A. Gharbi Stage I
- B. Gharbi Stage II
- C. Gharbi Stage III (Correct Answer)
- D. Gharbi Stage IV
Explanation: ***Gharbi Stage III*** - This stage is characterized by a **cystic lesion with internal floating membranes** (daughter cysts or detached endocyst), which is consistent with the "Water lily sign" described. - The membranes are indicative of a **degenerating or ruptured endocyst** within the main cyst, signifying a more advanced stage than simple cysts. *Gharbi Stage I* - This stage represents a **simple, unilocular cyst** with an anechoic (fluid-filled) lumen, without any internal structures or membranes. - It would appear as a clearly defined, fluid-filled mass with a smooth wall, lacking the internal complexity shown in the image. *Gharbi Stage II* - Gharbi Stage II is characterized by a **cyst with internal septations**, indicating the presence of multiple daughter cysts within the main cyst. - While it involves internal structures, these are typically well-defined septa rather than freely moving, detached membranes. *Gharbi Stage IV* - This stage describes a **heterogeneous, degenerating cyst** with a solid-like appearance, often without a clear cystic lumen. - It reflects a more advanced, often calcified or completely inactivated cyst, which does not match the clear cystic structure with floating membranes seen in the image.
Question 9: A man presents with back pain following a road traffic accident (RTA). There is no history of neurological deficit. An X-ray of the spine is done. What is the diagnosis based on the image?
- A. Spinous process fracture (Correct Answer)
- B. Chance fracture
- C. Compression fracture
- D. Fracture of base of vertebrae
Explanation: ***Spinous process fracture*** - The X-ray image reveals a **fracture of the spinous process** of one of the cervical vertebrae, characterized by a visible discontinuity or separation of this posterior bony projection. - This type of fracture, often caused by direct trauma or forceful hyperextension/hyperflexion, typically presents with localized back pain but often **without neurological deficit** as the spinal canal generally remains intact. *Chance fracture* - A **Chance fracture** (or seatbelt fracture) is a horizontal fracture of a vertebral body, usually in the thoracolumbar region, often caused by distractional forces (e.g., flexion over a seatbelt). - It involves all three columns of the spine (anterior, middle, and posterior) and is not seen in the cervical spine X-ray provided. *Compression fracture* - A **compression fracture** is characterized by the collapse of the vertebral body, often resulting in a wedge shape. - This typically appears as reduced height of the anterior vertebral body on an X-ray, which is not the primary finding in the image. *Fracture of base of vertebrae* - A **fracture at the base of the vertebrae** is a non-specific term; specific vertebral fractures are categorized based on the part of the vertebra affected (e.g., vertebral body, pedicle, lamina, spinous process). - The image distinctly shows a fracture in the **spinous process**, not the main body or base of the vertebra.
Question 10: Identify the condition shown in the given X-ray:
- A. Tibial tuberosity fracture
- B. Osgood-Schlatter disease (Correct Answer)
- C. Gerdy's tubercle fracture
- D. Lateral epicondyle of femur
Explanation: ***Correct Answer: Osgood-Schlatter disease*** - The X-ray shows characteristic **fragmentation** and **irregularity** of the **tibial tuberosity**, which is pathognomonic for Osgood-Schlatter disease. - This condition commonly affects **adolescents** during periods of rapid growth, causing **anterior knee pain** that worsens with activity. - The radiographic findings demonstrate chronic **traction apophysitis** at the insertion of the **patellar tendon**. *Incorrect: Tibial tuberosity fracture* - An acute tibial tuberosity fracture would show a **distinct fracture line** with possible displacement, rather than the chronic fragmentation pattern seen here. - This type of fracture typically results from **sudden forceful quadriceps contraction** and presents with acute onset of severe pain. *Incorrect: Gerdy's tubercle fracture* - Gerdy's tubercle is located on the **lateral aspect of the proximal tibia**, serving as the insertion point for the **iliotibial band**. - A fracture at this location would not explain the **anterior tibial tuberosity changes** visible in this X-ray image. *Incorrect: Lateral epicondyle of femur* - The lateral epicondyle of the femur is located at the **distal end of the femur**, not at the tibial tuberosity where the radiographic changes are visible. - Pathology at the lateral epicondyle would not cause the **tibial tuberosity fragmentation** seen in this X-ray.