All SubjectsAnatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q11
A 13-year-old boy presents with jaundice, fatigue, muscle stiffness, tremors, and behavioral changes. Examination reveals an enlarged liver and spleen. A Kayser-Fleischer ring was noted. What is the definitive diagnostic test?
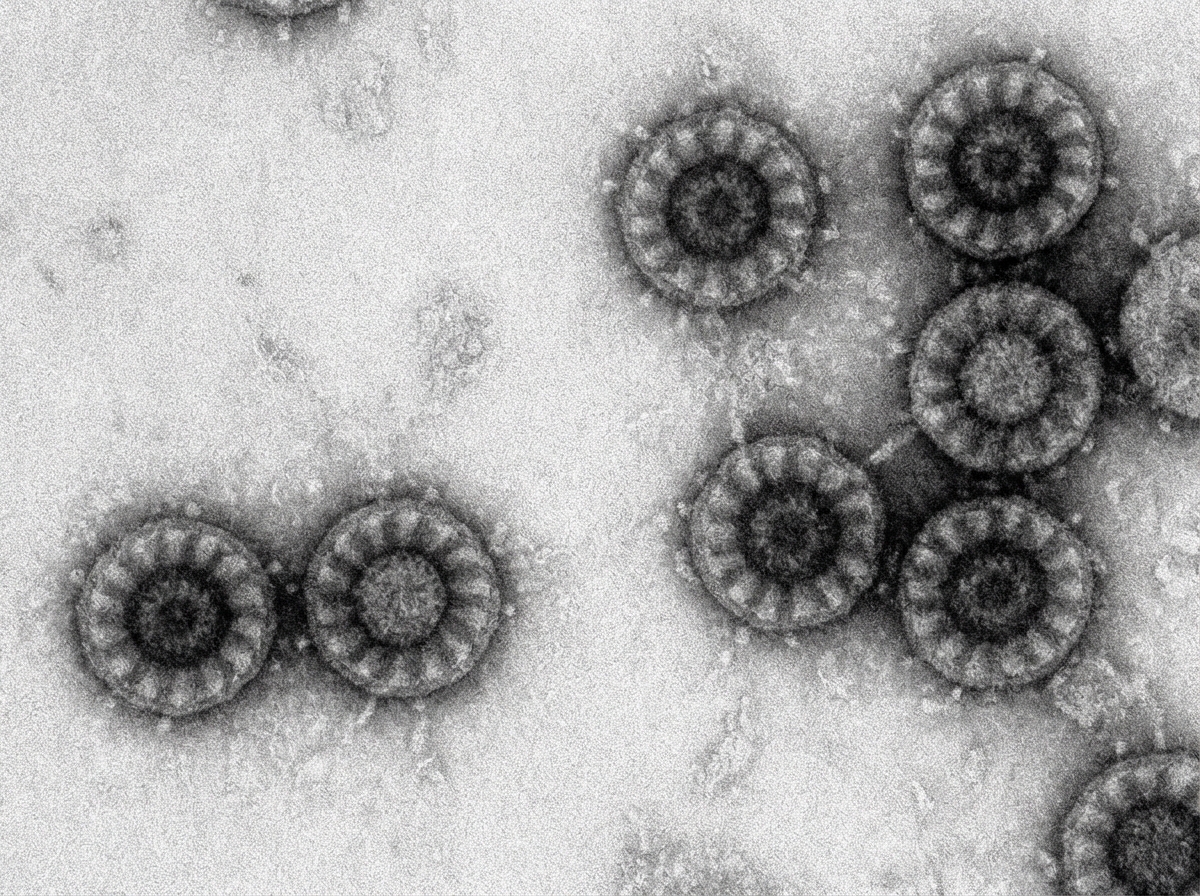
Q12
A 2 year old child came with watery diarrhea. Electron Microscopy (EM) Image is shown here. Choose the correct pathogen.
Q13
A 6-year-old child presents to the emergency department with sudden onset of palpitations, shortness of breath, and dizziness. The child has no significant past medical history. On examination, the heart rate is 220 beats per minute, blood pressure is $90 / 60 \mathrm{mmHg}$, and the child appears anxious but is otherwise stable. An ECG confirms the diagnosis of paroxysmal supraventricular tachycardia (PSVT). What is the initial recommended dose of adenosine for this child?
Q14
A child presents with recurrent infections. Mediastinal imaging reveals an absent thymus gland, and further investigations show low ADA (adenosine deaminase) levels. What is the most likely diagnosis?
Q15
A 2 -month-old child presents with the following condition as shown in the image. What is the ideal management protocol?

Q16
A baby presents with hydrocephalus, intracranial calcifications, and chorioretinitis. What is the most probable diagnosis?
Q17
A mother delivers in a rural area under the guidance of a skilled care attendant. Which of the following statements is incorrect regarding the care provided by the skilled care attendant at birth?
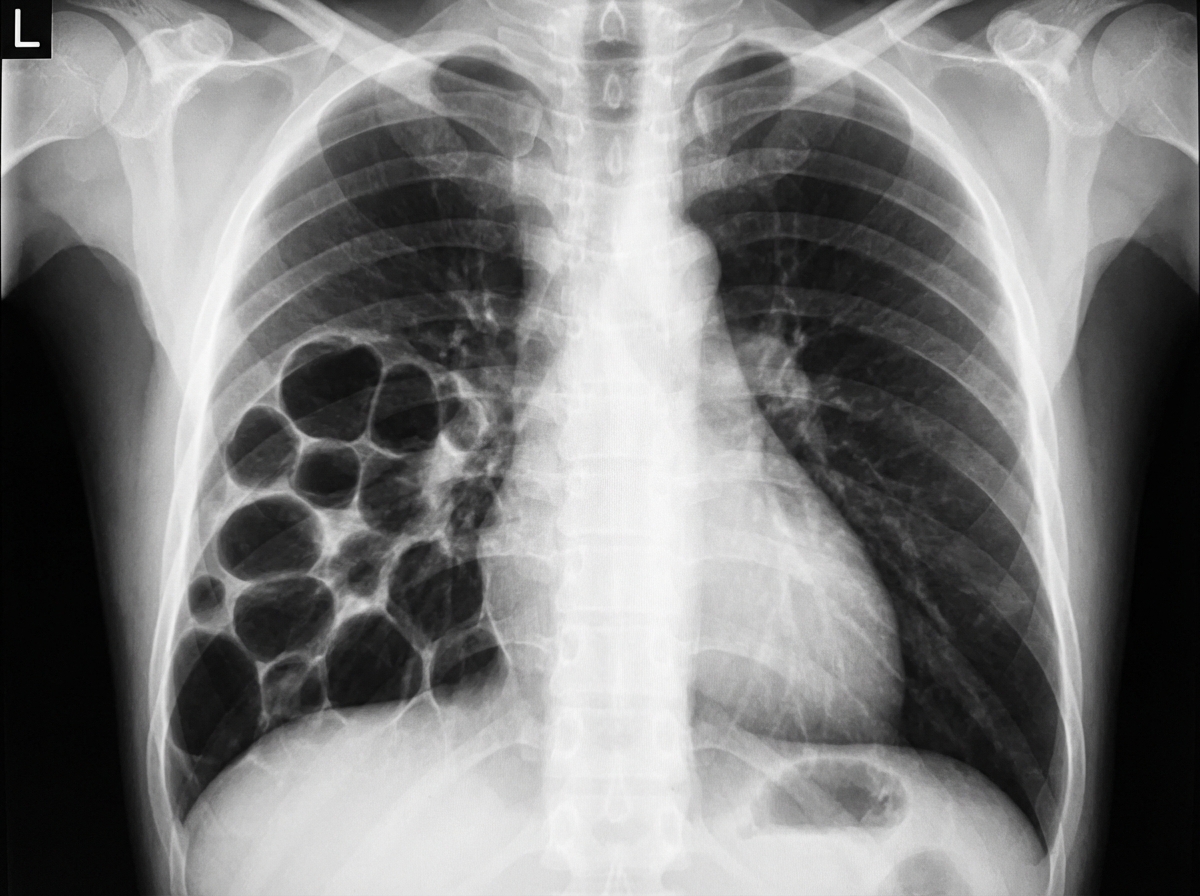
Q18
A 3-year-old child presents with respiratory distress and a history of recurrent respiratory infections. Based on the provided imaging, what is the most likely diagnosis?