NEET-PG 2024 — Pediatrics
18 Previous Year Questions with Answers & Explanations
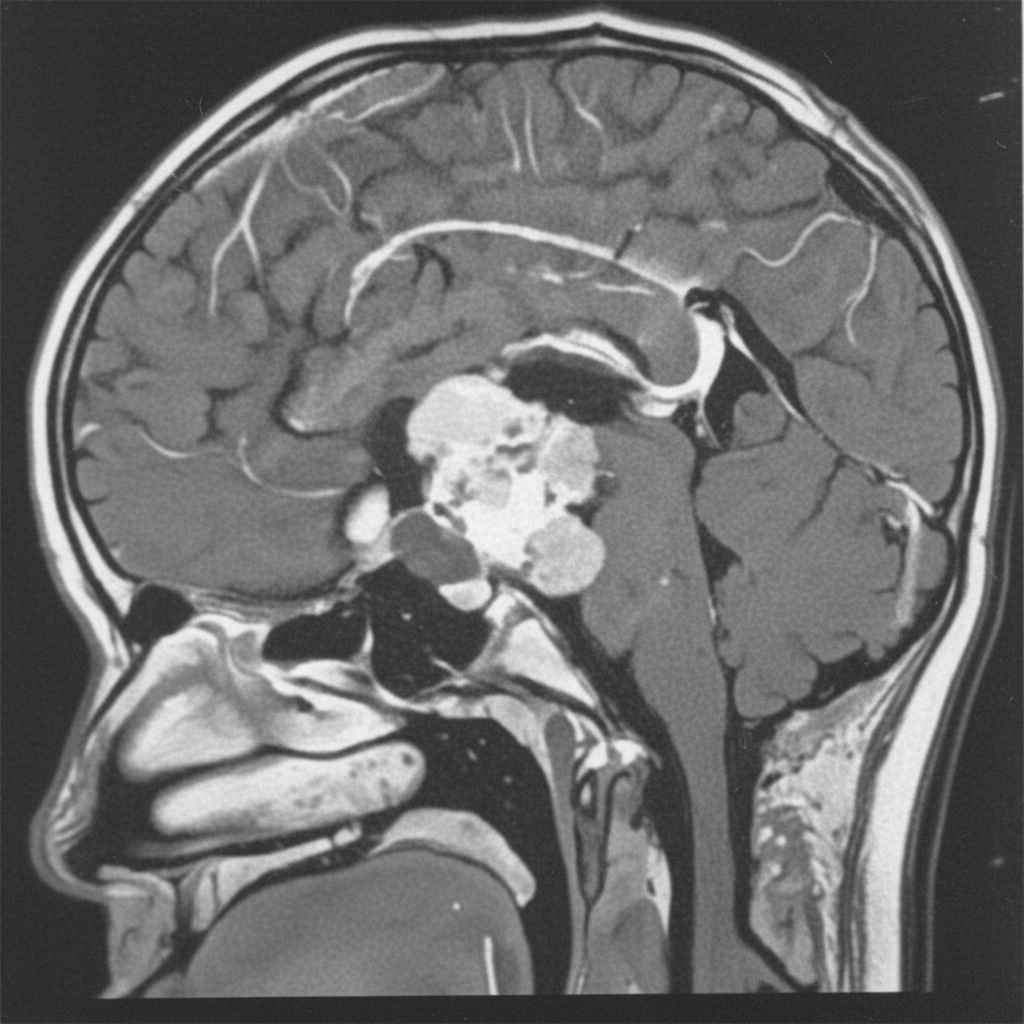
A 12-year-old boy presents with symptoms of headaches, visual disturbances, and growth retardation. An MRI scan is performed, and the image provided shows a cystic mass with both solid and calcified components in the suprasellar region, extending into the third ventricle. Based on the clinical presentation and MRI findings, what is the most likely diagnosis?
A 2-year-old boy presents with a history of recurrent urinary tract infections, poor urinary stream, and failure to thrive. A voiding cystourethrogram (VCUG) is performed, and the images provided show dilated posterior urethra and a thickened bladder wall with a keyhole appearance. Based on these findings, the diagnosis of posterior urethral valves (PUV) is made. What is the management for this condition?
A 6-week-old child with a history of vomiting undergoes an ultrasound, which shows an antral nipple sign or target sign, as shown in the image. What is the diagnosis?
A 3-year-old child presents to the OPD with a history of recurrent urinary tract infections, poor urinary stream, and difficulty voiding. The radiological image is shown below. What is the most appropriate management?
An unimmunized 5 -year-old child presents to the OPD with a white membranous layer on the throat upon inspection. The child's brother is immunized. What is the first step in management?
An unimmunized 5 -year-old child presents to the OPD with a white membranous layer on inspection, suggesting diphtheria. What is the appropriate prophylaxis for a 2 -year-old contact who has completed their vaccination?
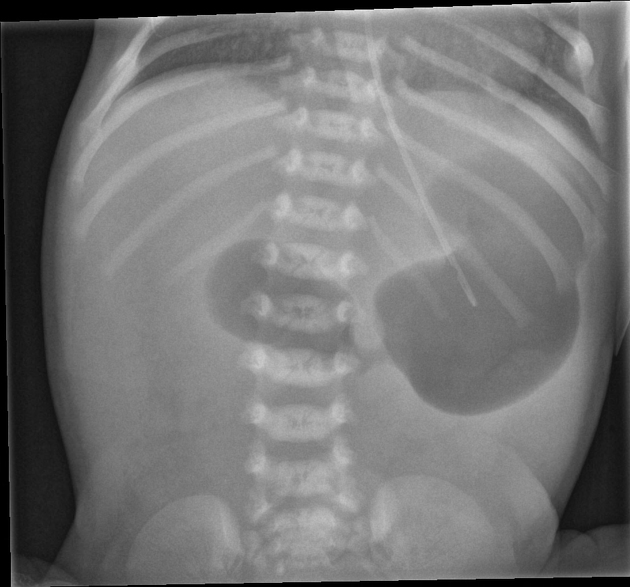
A 6-week-old baby is brought in by the mother with complaints of vomiting. An X-ray shows a single bubble appearance. What is the most likely diagnosis?
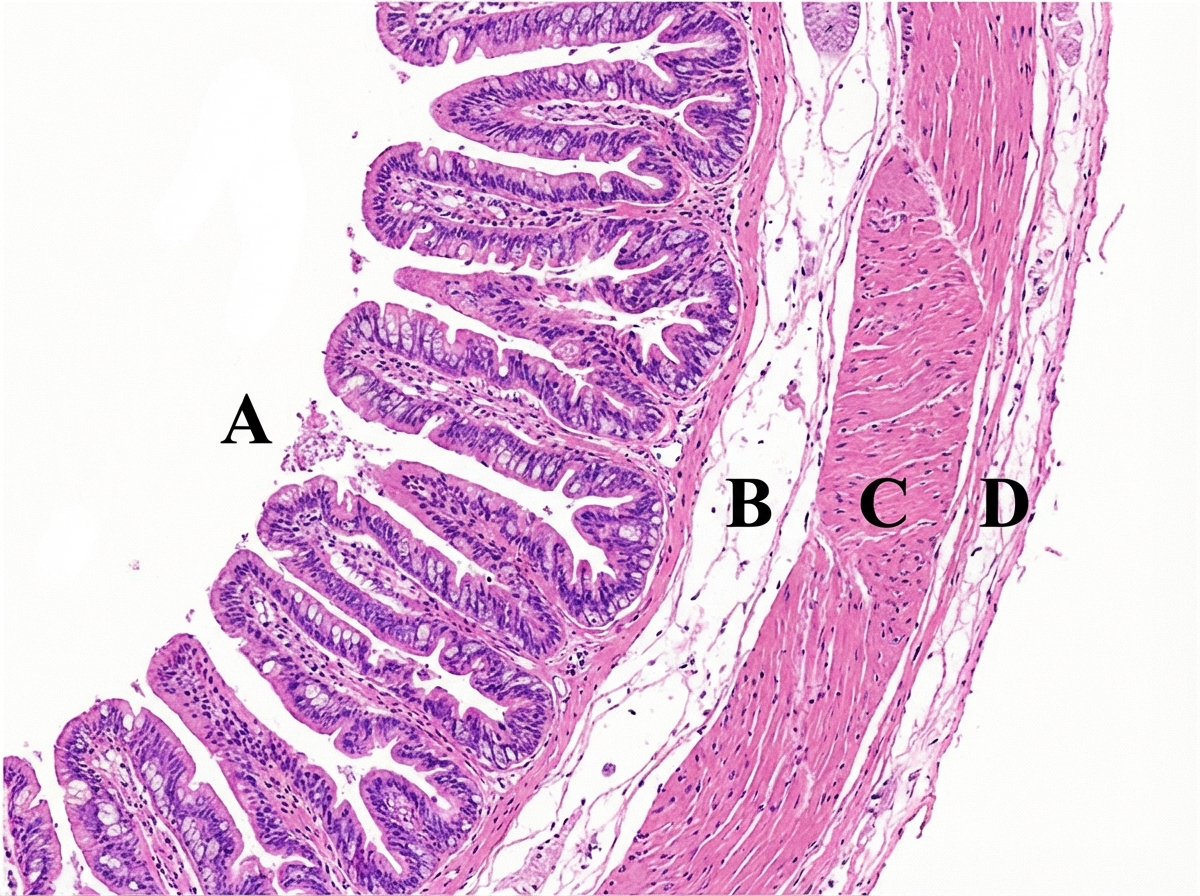
A neonate presents with failure to pass meconium. The structure absent in the pathology lies in which of the following layers?
What is the diagnosis based on the image shown 

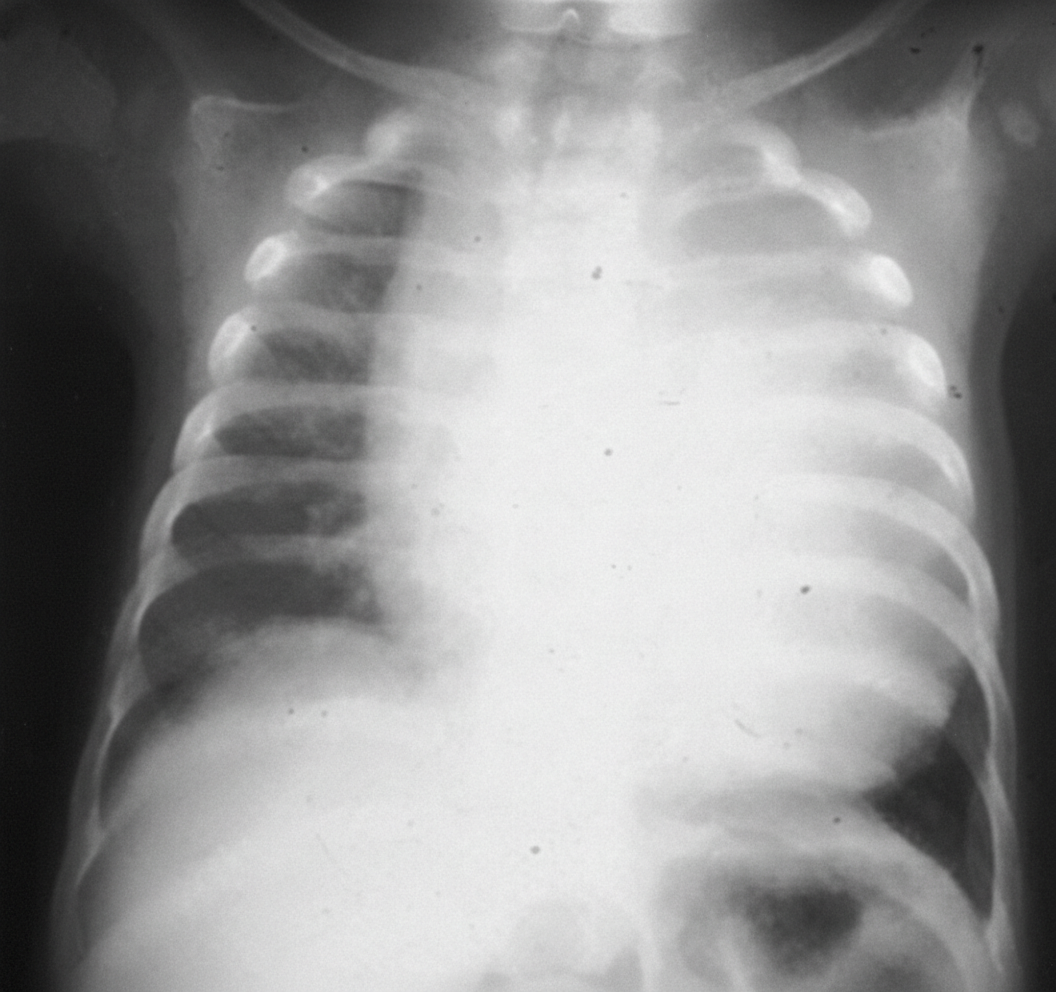
A patient presents with an X-ray showing cardiomegaly, along with symptoms of hypotonia, macroglossia, hepatomegaly, and floppy baby syndrome. The X ray of the infant is shown below. What is the most likely diagnosis?
NEET-PG 2024 - Pediatrics NEET-PG Practice Questions and MCQs
Question 1: A 12-year-old boy presents with symptoms of headaches, visual disturbances, and growth retardation. An MRI scan is performed, and the image provided shows a cystic mass with both solid and calcified components in the suprasellar region, extending into the third ventricle. Based on the clinical presentation and MRI findings, what is the most likely diagnosis?
- A. Craniopharyngioma (Correct Answer)
- B. Germinoma
- C. Meningioma
- D. Pituitary adenoma
- E. Optic glioma
Explanation: ***Craniopharyngioma*** - This tumor is classically described as having **cystic** and **solid components** with **calcification**, which is evident in the provided MRI image. Its location in the **suprasellar region** and extension into the **third ventricle** are also typical. - The clinical presentation of **headaches**, **visual disturbances** (due to compression of the optic chiasm), and **growth retardation** (due to hypothalamic-pituitary axis dysfunction) in a 12-year-old boy is highly suggestive of a craniopharyngioma, which commonly affects children and young adults. *Germinoma* - While germinomas can occur in the suprasellar region and cause similar endocrine and visual symptoms, they typically appear as **solid, homogeneously enhancing masses** on MRI and are less commonly cystic and calcified. - They are more common in adolescence and are highly sensitive to radiation therapy, but their imaging characteristics differ from the described lesion. *Meningioma* - Meningiomas typically arise from the **arachnoid mater** and are usually **solid, extra-axial masses** that often have a **dural tail sign** on MRI. - They are less common in children, and while they can calcify, their characteristic imaging features (extra-axial, dural attachment) are not consistent with the described suprasellar, intra-axial cystic mass. *Pituitary adenoma* - Pituitary adenomas originate from the **pituitary gland** and are usually located within the sella turcica, extending superiorly. While they can be cystic, **calcification is rare**, and they are more commonly solid and homogeneously enhancing. - Although they can cause visual disturbances and hormonal imbalances, the prominent cystic-solid appearance with calcification and clear suprasellar origin extending into the third ventricle makes craniopharyngioma a more likely diagnosis in this age group and imaging. *Optic glioma* - Optic gliomas (pilocytic astrocytomas) are common **suprasellar tumors in children**, especially those with neurofibromatosis type 1, and can cause visual disturbances and endocrine dysfunction. - However, they typically appear as **solid, fusiform masses** involving the optic nerve or chiasm with **homogeneous enhancement** and rarely show the characteristic cystic-solid architecture with prominent calcification seen in craniopharyngiomas.
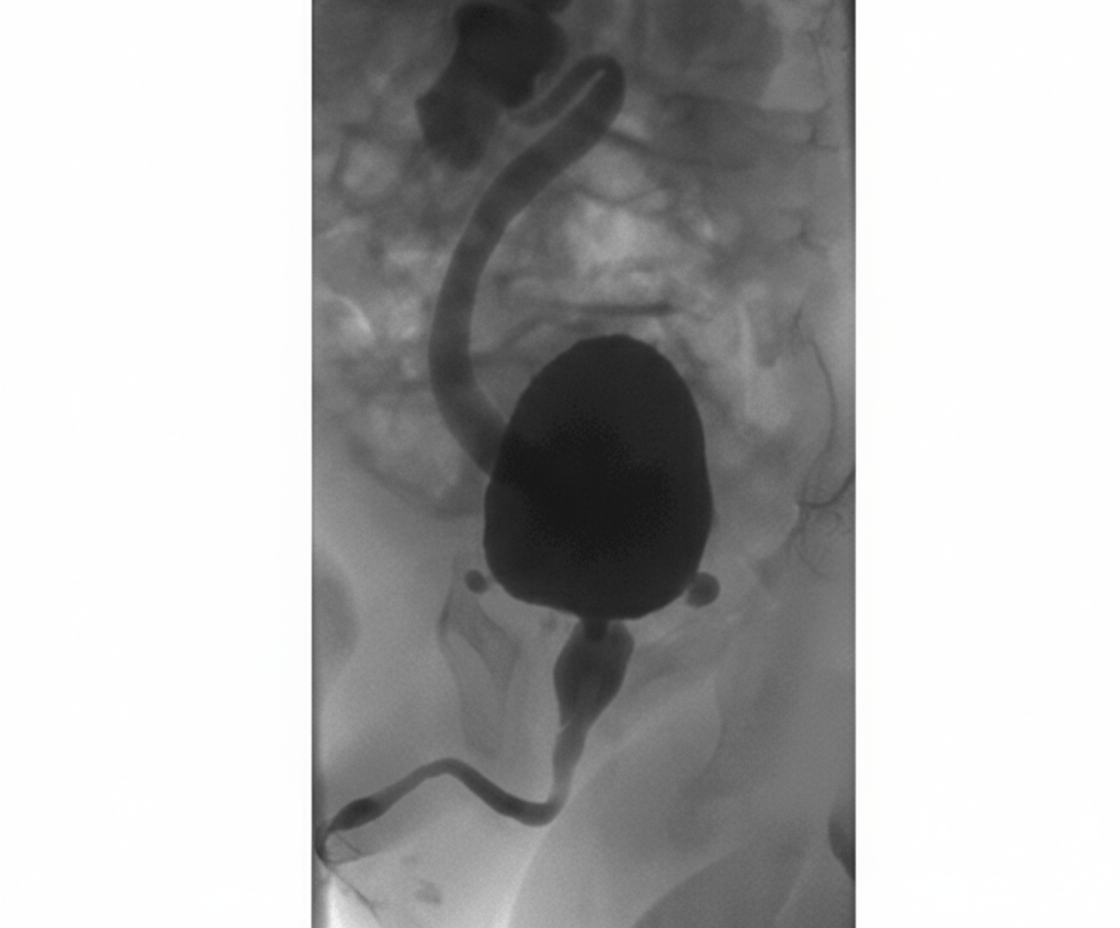
Question 2: A 2-year-old boy presents with a history of recurrent urinary tract infections, poor urinary stream, and failure to thrive. A voiding cystourethrogram (VCUG) is performed, and the images provided show dilated posterior urethra and a thickened bladder wall with a keyhole appearance. Based on these findings, the diagnosis of posterior urethral valves (PUV) is made. What is the management for this condition?
- A. Antibiotic prophylaxis and monitoring
- B. Endoscopic valve ablation (Correct Answer)
- C. Suprapubic cystostomy
- D. Observation with follow-up imaging
- E. Urinary diversion with vesicostomy
Explanation: ***Endoscopic valve ablation*** - This is the **definitive treatment** for posterior urethral valves (PUV) as it directly addresses the anatomical obstruction. - Ablating the valves with a **cystoscope** relieves the outflow obstruction, preventing further damage to the bladder and kidneys. *Antibiotic prophylaxis and monitoring* - While important for managing recurrent UTIs and preventing future infections in children with PUV, it does **not address the underlying anatomical obstruction**. - Without surgical intervention, the obstruction would persist, leading to progressive urinary tract damage despite antibiotic use. *Suprapubic cystostomy* - This procedure involves placing a catheter directly into the bladder via the abdominal wall to **divert urine**. - It is typically a **temporary measure** used for initial decompression in severely ill patients or those with complete obstruction, not the definitive management. *Urinary diversion with vesicostomy* - Vesicostomy creates an opening between the bladder and abdominal wall for temporary urinary diversion. - This may be used in **very young infants** or critically ill patients as a temporizing measure, but **endoscopic ablation remains the definitive treatment**. *Observation with follow-up imaging* - **Observation is not appropriate** for symptomatic PUV due to the risk of progressive and irreversible renal damage. - The condition requires **prompt intervention** to relieve the obstruction and prevent long-term complications like renal failure.
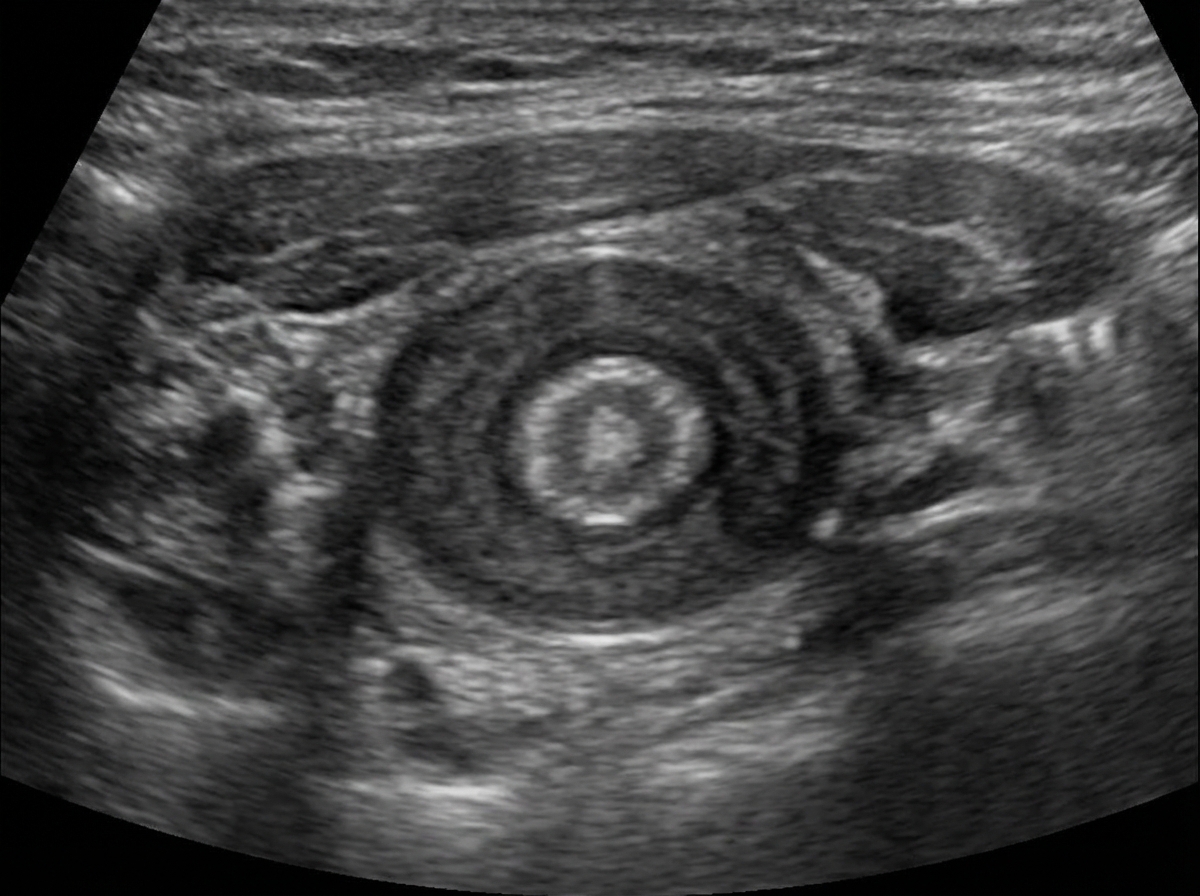
Question 3: A 6-week-old child with a history of vomiting undergoes an ultrasound, which shows an antral nipple sign or target sign, as shown in the image. What is the diagnosis?
- A. Congenital pyloric stenosis (Correct Answer)
- B. Umbilical hernia
- C. Small bowel obstruction
- D. Jejunal atresia
- E. Duodenal atresia
Explanation: ***Congenital pyloric stenosis*** - The ultrasound findings of an **antral nipple sign** and **target sign** are classic indicators of **hypertrophic pyloric stenosis**. - This condition presents with **projectile vomiting** in infants, typically between 3-6 weeks of age, due to hypertrophy of the pyloric muscle. *Umbilical hernia* - An **umbilical hernia** is a protrusion of abdominal contents through the umbilical ring. It is usually diagnosed clinically and presents as a bulge, not with vomiting. - Ultrasound for an umbilical hernia would show bowel loops or omentum protruding through the abdominal wall defect, not the specific pyloric signs described. *Small bowel obstruction* - While small bowel obstruction can cause vomiting, the ultrasound findings would typically show **dilated loops of bowel** and a **transition point**, not an antral nipple or target sign specifically at the pylorus. - Other clinical features, such as abdominal distention and absence of stool, would also be more prominent. *Jejunal atresia* - **Jejunal atresia** is a congenital anomaly where part of the jejunum is underdeveloped or absent, leading to a complete obstruction. - Ultrasound would reveal **dilated loops of small bowel**, typically without peristalsis past the obstruction, and polyhydramnios antenatally, but not the specific pyloric ultrasound signs. *Duodenal atresia* - **Duodenal atresia** is a congenital obstruction of the duodenum that typically presents with bilious vomiting soon after birth. - The characteristic ultrasound finding is the **"double bubble" sign**, representing a distended stomach and proximal duodenum, not the target or antral nipple sign seen at the pylorus.
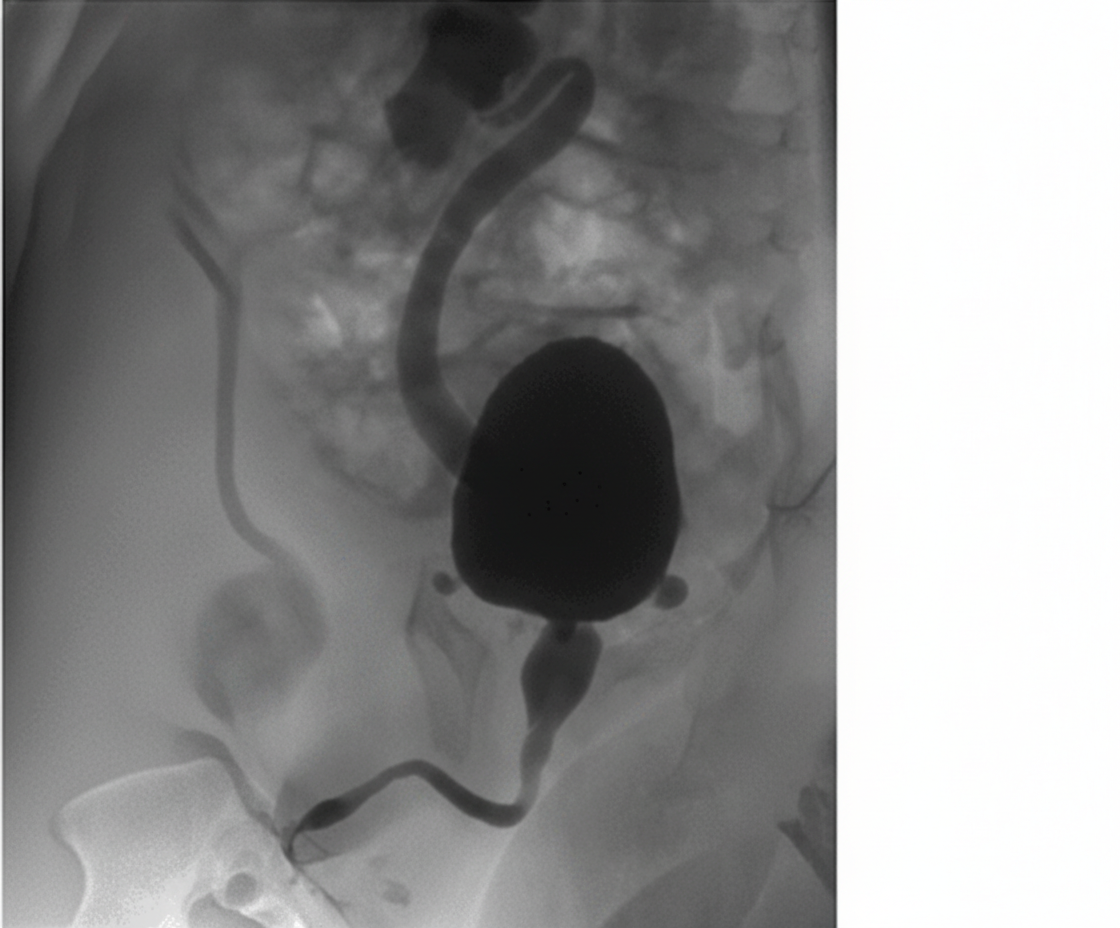
Question 4: A 3-year-old child presents to the OPD with a history of recurrent urinary tract infections, poor urinary stream, and difficulty voiding. The radiological image is shown below. What is the most appropriate management?
- A. Endoscopic ablation (Correct Answer)
- B. Dilation of urethra
- C. Dilation of urethra and bladder
- D. Conservative
- E. Vesicostomy
Explanation: ***Endoscopic ablation*** - The image shows a distended bladder with a dilated, elongated posterior urethra and a narrow stream of contrast beyond the bladder neck, characteristic findings of **posterior urethral valves (PUV)**. - **Endoscopic ablation (incision or fulguration)** of the valves is the definitive treatment for PUV to relieve obstruction and prevent further kidney damage. - This is the **gold standard primary treatment** for PUV in children who are large enough to undergo the procedure safely. *Dilation of urethra* - **Dilation** is generally ineffective because PUV are folds of tissue that require incision rather than simple stretching. - This approach does not address the underlying anatomical obstruction caused by the valves and could potentially cause damage to the urethra. *Dilation of urethra and bladder* - **Dilation of the urethra** is not an effective treatment for PUV. The bladder is already dilated due to the obstruction, and further dilation would not resolve the issue. - This approach would not remove the obstruction and could worsen bladder function or lead to further complications like reflux. *Conservative* - **Conservative management** with watchful waiting is not appropriate for PUV, as untreated obstruction can lead to progressive and irreversible kidney damage, bladder dysfunction, and recurrent UTIs. - Timely intervention is crucial to preserve renal function and improve long-term outcomes in boys with PUV. *Vesicostomy* - **Vesicostomy** (temporary bladder diversion) is reserved for specific scenarios such as neonates or very young infants too small for safe endoscopic ablation, severe hydronephrosis with renal failure, or failed primary ablation. - In this **3-year-old child**, endoscopic ablation is preferred as the primary definitive treatment rather than temporary diversion, which would require a second procedure later.
Question 5: An unimmunized 5 -year-old child presents to the OPD with a white membranous layer on the throat upon inspection. The child's brother is immunized. What is the first step in management?
- A. Diphtheria antitoxin (Correct Answer)
- B. Diphtheria toxoid
- C. Penicillin
- D. Isolation and supportive care
- E. Tracheostomy
Explanation: ***Diphtheria antitoxin*** - The presence of a **white membranous layer** on the **throat** in an **unimmunized child**, along with the high contagiousness (brother's immunization is relevant to exposure), strongly suggests **diphtheria**. - **Diphtheria antitoxin (DAT)** is the crucial first-line treatment to neutralize the **exotoxin** produced by *Corynebacterium diphtheriae*, which is responsible for the severe systemic effects. - Antitoxin must be administered **immediately** without waiting for culture confirmation, as it only neutralizes unbound toxin. *Diphtheria toxoid* - **Diphtheria toxoid** is used for **active immunization** (vaccination) to prevent diphtheria, not for emergency treatment of an active infection. - Administering toxoid during an acute infection would not rapidly neutralize the circulating toxin. *Penicillin* - **Penicillin** (or erythromycin) is used to **eradicate the bacteria** (*Corynebacterium diphtheriae*) from the patient's throat and prevent further toxin production and transmission. - While important for source control, it does not neutralize the pre-formed toxin, which is the immediate threat to life. - Antibiotics should be given **after** antitoxin administration. *Isolation and supportive care* - **Isolation** is essential to prevent transmission, but it does not treat the patient's infection. - **Supportive care** is also crucial, but it addresses symptoms rather than the underlying cause or the effects of the toxin. *Tracheostomy* - **Tracheostomy** may be required later for airway obstruction if the membrane extends to the larynx or causes significant respiratory compromise. - However, it is **not the first step** in management; securing airway patency comes after antitoxin administration unless there is immediate life-threatening airway obstruction. - The priority is neutralizing the toxin to prevent further membrane formation and systemic complications.
Question 6: An unimmunized 5 -year-old child presents to the OPD with a white membranous layer on inspection, suggesting diphtheria. What is the appropriate prophylaxis for a 2 -year-old contact who has completed their vaccination?
- A. No prophylaxis needed
- B. Toxoid
- C. Immunoglobulins
- D. Penicillin (Correct Answer)
- E. Erythromycin
Explanation: ***Penicillin*** - For a **fully vaccinated contact** of a diphtheria case, **antibiotic prophylaxis** (e.g., penicillin or erythromycin) is recommended to prevent carriage and transmission of *Corynebacterium diphtheriae*. - This approach aims to eradicate the organism from the respiratory tract, even if the contact is otherwise protected from the disease itself. - **Penicillin** is a commonly used first-line agent for this purpose. *Erythromycin* - **Erythromycin** is also an acceptable antibiotic for diphtheria prophylaxis and is particularly useful in penicillin-allergic patients. - Both penicillin and erythromycin are effective for preventing carriage; the choice between them may depend on local guidelines, patient allergies, and availability. - In this context, either would be clinically appropriate, but penicillin is often listed as the primary option in standard guidelines. *No prophylaxis needed* - This is incorrect because even vaccinated individuals can become **asymptomatic carriers** of *C. diphtheriae* and transmit the infection to unimmunized or under-immunized contacts. - Prophylaxis is crucial for **breaking the chain of transmission** in a household or close contact setting. *Toxoid* - **Diphtheria toxoid** is the active component of the diphtheria vaccine, which stimulates the immune system to produce antibodies against diphtheria toxin, preventing the disease. - While important for ongoing immunity, administering the toxoid as an immediate prophylaxis for a fully vaccinated contact is not the primary intervention for preventing carriage; **antibiotics are used for this purpose**. *Immunoglobulins* - **Diphtheria antitoxin** (DAT), which contains immunoglobulins, is used for the **treatment of active diphtheria disease** by neutralizing the circulating toxin. - It is not indicated for prophylaxis in vaccinated contacts, as their immune system is already primed to handle potential exposure to the toxin, and the goal of prophylaxis here is to prevent colonization rather than toxin effects.
Question 7: A 6-week-old baby is brought in by the mother with complaints of vomiting. An X-ray shows a single bubble appearance. What is the most likely diagnosis?
- A. Duodenal atresia
- B. Annular pancreas
- C. Congenital hypertrophic pyloric stenosis (CHPS) (Correct Answer)
- D. Jejunal atresia
- E. Malrotation with midgut volvulus
Explanation: ***Congenital hypertrophic pyloric stenosis (CHPS)*** - The **single bubble appearance** observed in the X-ray, along with vomiting in a 6-week-old, is characteristic of an obstruction at the gastric outlet due to **pyloric stenosis**. The "bubble" represents the dilated stomach. - Infants with CHPS typically present with **non-bilious projectile vomiting** around 3-6 weeks of age, often accompanied by good appetite. *Duodenal atresia* - This condition classically presents with a **"double bubble" sign** on X-ray, representing dilation of the stomach and the proximal duodenum. - Vomiting is usually **bilious** and occurs earlier, often from birth. *Annular pancreas* - Annular pancreas can cause duodenal obstruction, leading to a **"double bubble" sign** similar to duodenal atresia. - The presentation would also be earlier, typically with **bilious vomiting** from birth or shortly thereafter. *Jejunal atresia* - Jejunal atresia would result in **multiple dilated loops of small bowel** proximal to the obstruction with air-fluid levels, rather than a single bubble. - The vomiting would be **bilious** and abdominal distension would be more prominent. *Malrotation with midgut volvulus* - This presents with **bilious vomiting** and can occur at any age, though commonly in the first few weeks of life. - X-ray findings include a **"corkscrew" or "whirl" sign** on contrast studies, or a gasless abdomen if complete obstruction occurs. - Unlike the single bubble of pyloric stenosis, malrotation typically shows abnormal bowel gas patterns or a paucity of gas in the abdomen.
Question 8: A neonate presents with failure to pass meconium. The structure absent in the pathology lies in which of the following layers?
- A. A, B
- B. B, C
- C. C, D (Correct Answer)
- D. A, D
- E. B, D
Explanation: ***C, D*** - The neonate's symptom of **failure to pass meconium** is characteristic of **Hirschsprung disease**, which is caused by the absence of **ganglion cells** in the distal colon. - The missing ganglion cells are typically found in the **submucosal (Meissner) plexus** and the **myenteric (Auerbach) plexus**, corresponding to layers C and D in the provided image. *A, B* - Layer A represents the **mucosa** (specifically the glandular epithelium), and layer B represents the **lamina propria** or potentially the muscularis mucosa. - These layers do not primarily house the ganglion cells implicated in Hirschsprung disease. *B, C* - Layer B is the **lamina propria** or **muscularis mucosa**, and layer C is the **submucosa**. - While the submucosa (C) contains the Meissner plexus, layer B does not contain ganglion cells relevant to this pathology. *B, D* - Layer B is the **lamina propria/muscularis mucosa**, and layer D is the **muscularis propria**. - While the myenteric plexus (associated with D) is affected in Hirschsprung disease, layer B does not contain ganglion cells, and this option incorrectly excludes the submucosal plexus (layer C), which also contains ganglion cells that are absent in this condition. *A, D* - Layer A is the **mucosa**, and layer D is the **muscularis propria** (outer muscle layer). - The mucosa (A) does not contain the ganglion cells, while the myenteric plexus (associated with D) is affected, but this option incorrectly includes A and omits the submucosal plexus (C).
Question 9: What is the diagnosis based on the image shown 
- A. Bladder exstrophy (Correct Answer)
- B. Omphalocele
- C. Umbilical hernia
- D. Gastroschisis
- E. Epispadias
Explanation: ***Bladder exstrophy*** - The image distinctly shows an **exposed urinary bladder** on the abdominal wall, a hallmark of bladder exstrophy. - This congenital anomaly results from a **failure of midline closure** of the infraumbilical abdominal wall and bladder. *Omphalocele* - An omphalocele involves protrusion of **abdominal viscera** (intestines, liver) into the base of the umbilical cord. - The herniated organs are typically **covered by a sac** composed of peritoneum and amnion, which is absent in the image. *Umbilical hernia* - An umbilical hernia is a protrusion of abdominal contents through the **umbilical ring**, but the skin remains intact and covers the defect. - The image clearly shows an **exposed organ** without skin coverage, ruling out an umbilical hernia. *Gastroschisis* - Gastroschisis involves the **evisceration of intestines** through a full-thickness abdominal wall defect, usually to the right of the umbilical cord. - Unlike the image, the defect in gastroschisis is typically **much smaller** and primarily involves the bowel, not the bladder, and there is no covering sac. *Epispadias* - Epispadias is a **urethral defect** where the urethral opening is on the dorsal (upper) surface of the penis or anterior bladder neck. - While epispadias is part of the **exstrophy-epispadias complex** and often associated with bladder exstrophy, it does not present with an **exposed bladder** on the abdominal wall as seen in the image.
Question 10: A patient presents with an X-ray showing cardiomegaly, along with symptoms of hypotonia, macroglossia, hepatomegaly, and floppy baby syndrome. The X ray of the infant is shown below. What is the most likely diagnosis?
- A. Pompe's disease (Correct Answer)
- B. Ebstein anomaly
- C. Transposition of great arteries
- D. Von Gierke's disease
- E. Congenital hypothyroidism
Explanation: ***Pompe's disease*** - Pompe's disease (Type II glycogen storage disease) is characterized by a deficiency of **alpha-glucosidase**, leading to **glycogen accumulation** in lysosomes. - This accumulation results in **cardiomegaly**, **hypotonia** ("floppy baby"), **hepatomegaly**, and **macroglossia**, which perfectly match the clinical presentation. *Ebstein anomaly* - This is a congenital heart defect involving the **tricuspid valve**, leading to its displacement into the right ventricle. - While it causes cardiomegaly, it does not typically present with the systemic features like **hypotonia, macroglossia, or hepatomegaly** described. *Transposition of great arteries* - This is a complex congenital heart defect where the **aorta and pulmonary artery are switched**, resulting in two separate circulatory systems. - It causes severe cyanosis and cardiomegaly but does not explain the widespread glycogen storage symptoms such as **hypotonia** or **hepatomegaly**. *Von Gierke's disease* - **Von Gierke's disease** (Type I glycogen storage disease) is caused by a deficiency of **glucose-6-phosphatase**. - It primarily affects the **liver and kidneys**, causing severe hypoglycemia, hepatomegaly, and **nephromegaly**, but typically not significant cardiomegaly or profound hypotonia. *Congenital hypothyroidism* - Can present with **macroglossia, hypotonia, and hepatomegaly** similar to Pompe's disease. - However, the **massive cardiomegaly** seen on X-ray is not typical of hypothyroidism, and other features like prolonged jaundice, constipation, and umbilical hernia would be more prominent.