All SubjectsAnatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q11
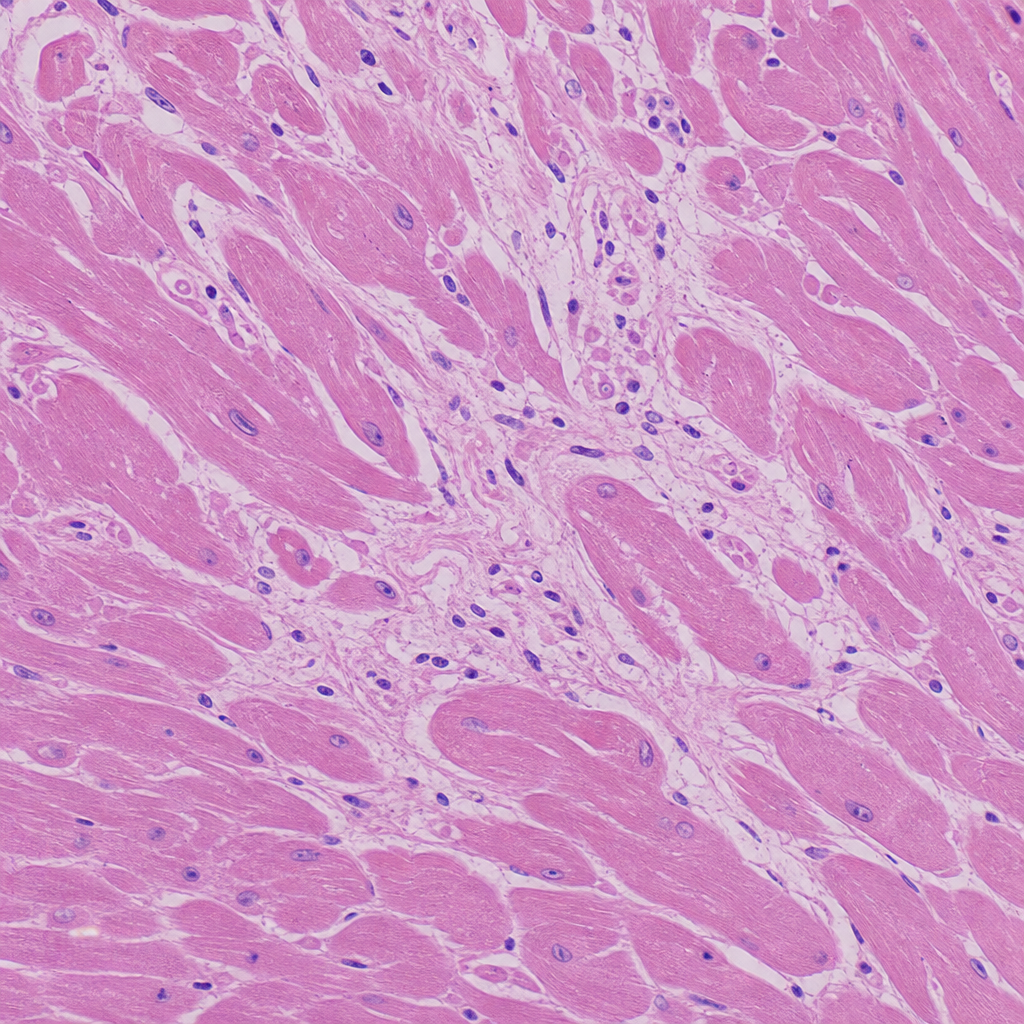
A 30-year-old football player presented to the emergency department with sudden cardiac arrest/collapse. Based on the histological image provided, what is the most likely cause of his death?
Q12
The skin biopsy shown below is most consistent with which of the following conditions? 
Q13
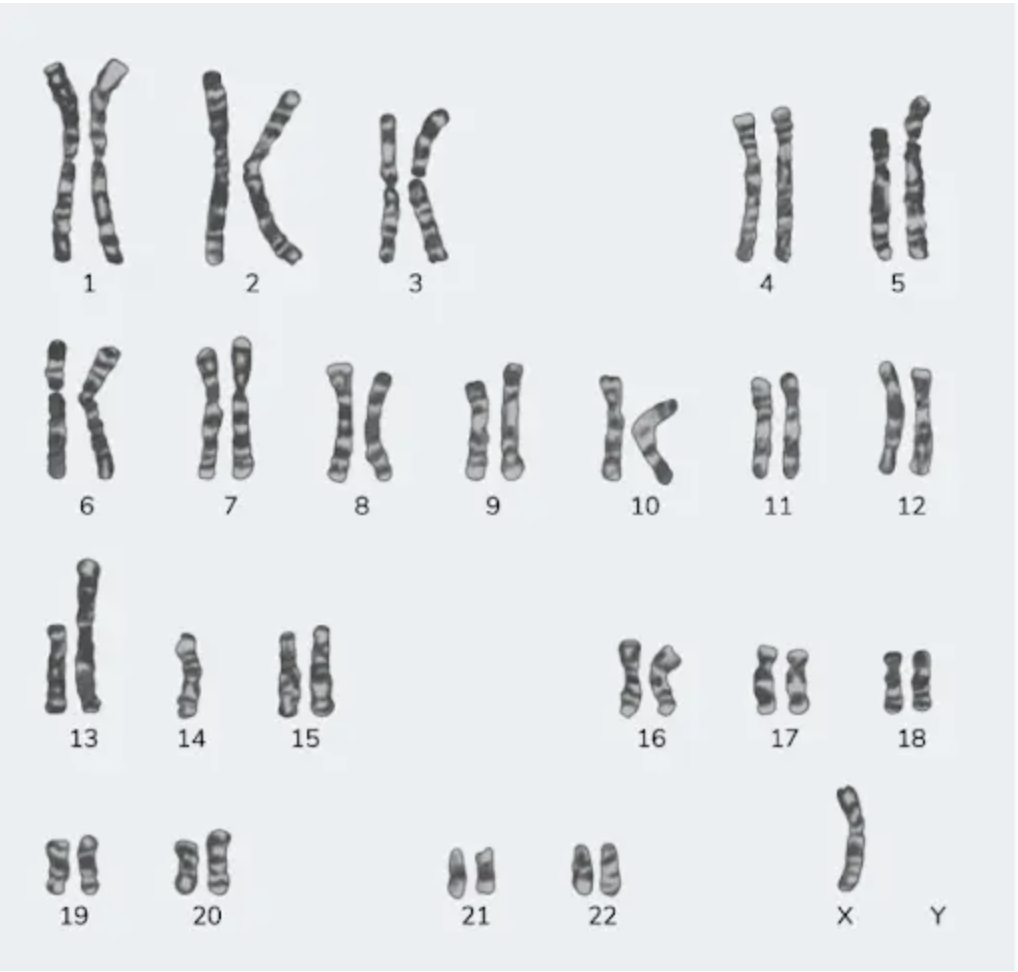
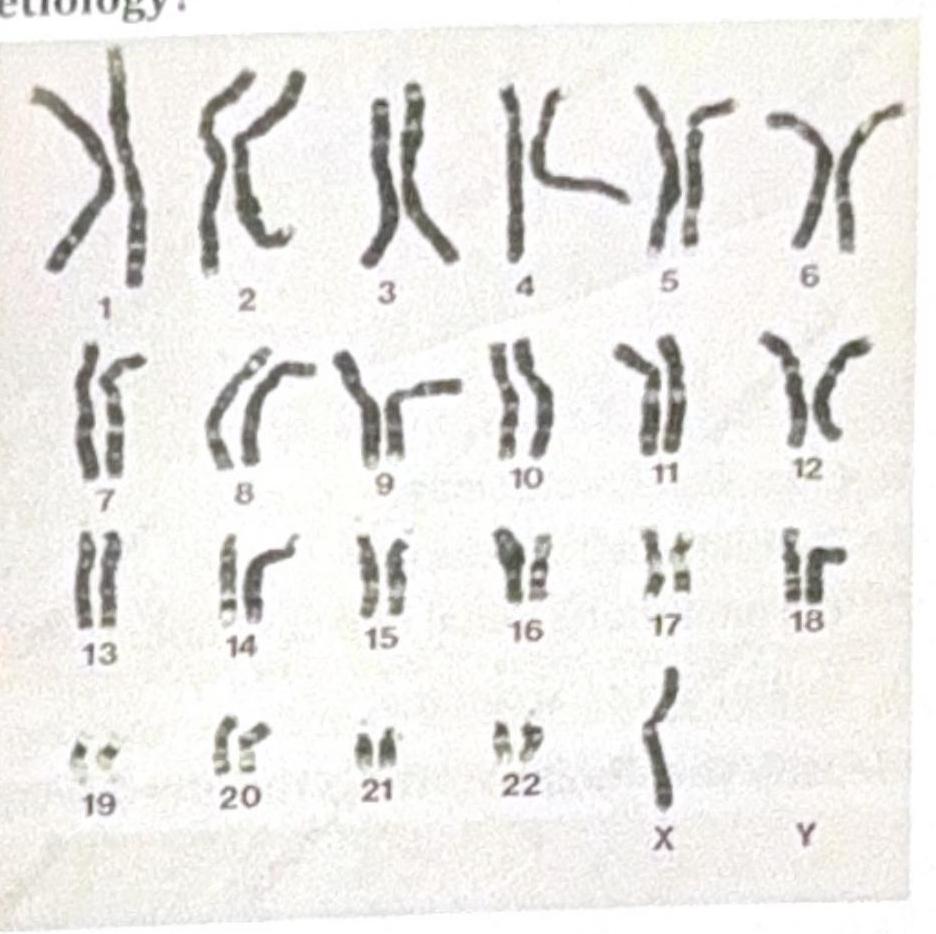
A 23-year-old female with a height of 4 feet has a karyotype as shown in the image below. Which among the following indicates the correct etiology?
Q14
The histopathology image shown is characteristic of which of the following diseases? 
Q15
A male patient is not responding to oxygen therapy and has been diagnosed with ARDS (Acute Respiratory Distress Syndrome). What is the role of IL-8 in ARDS?
Q16
A patient presents with respiratory distress and is diagnosed with panacinar emphysema. Which of the following is deficient?
Q17
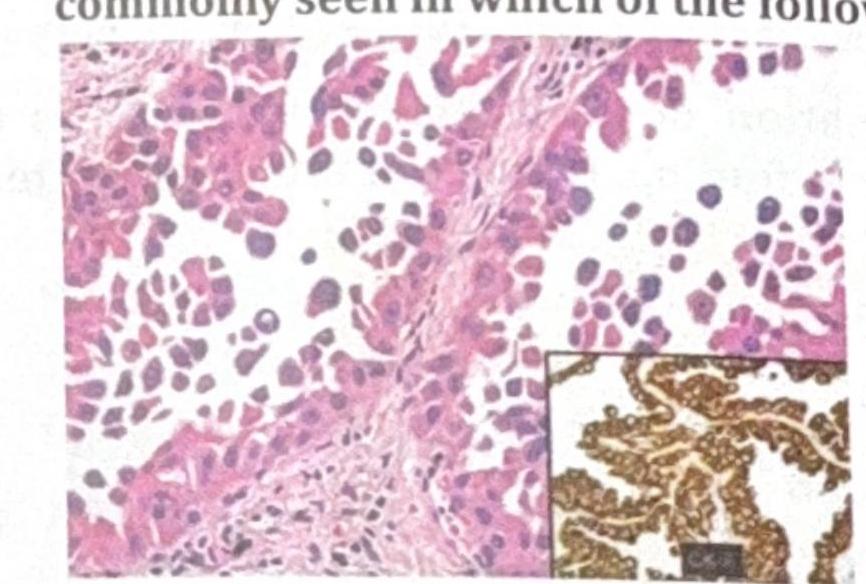
A patient presents with a renal mass leading to hematuria and flank pain. The histological image below is shown. What is the likely diagnosis?
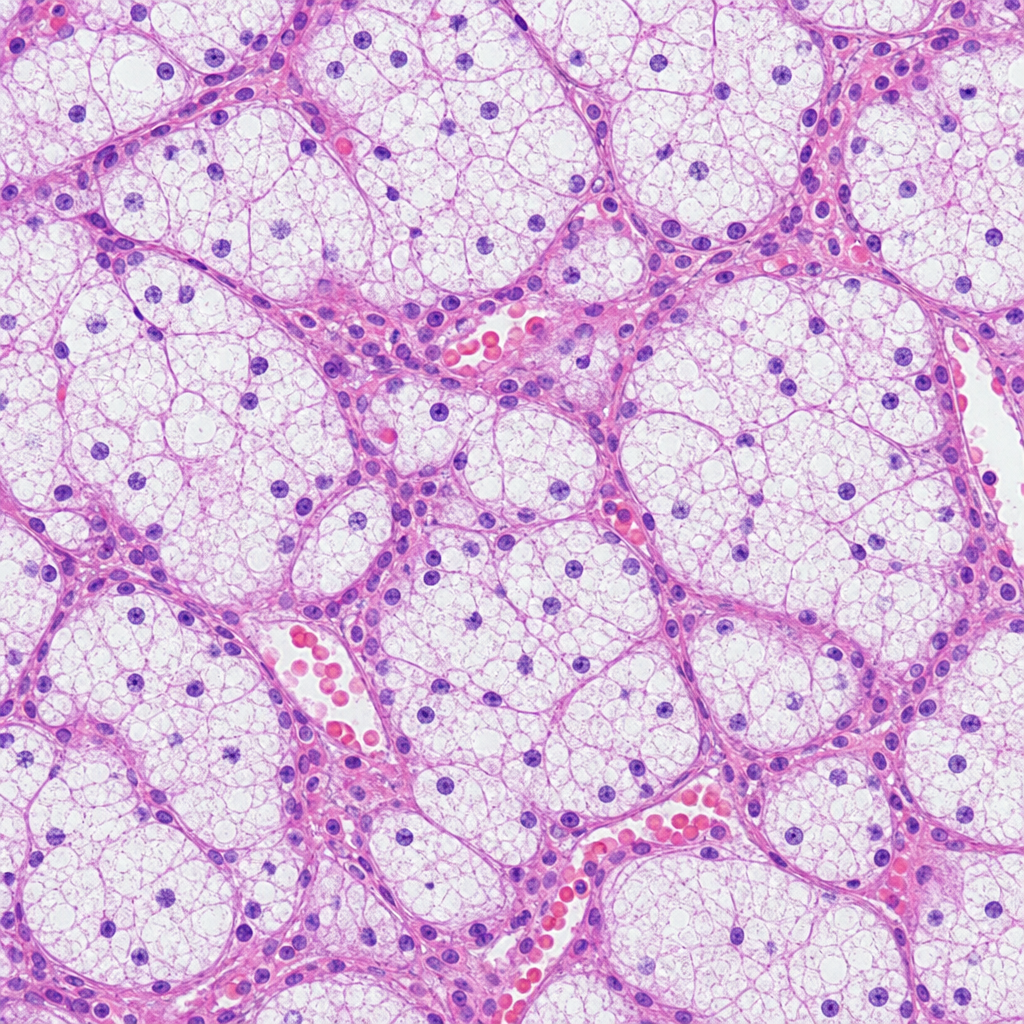
Q18
Identify the diagnosis from the given image
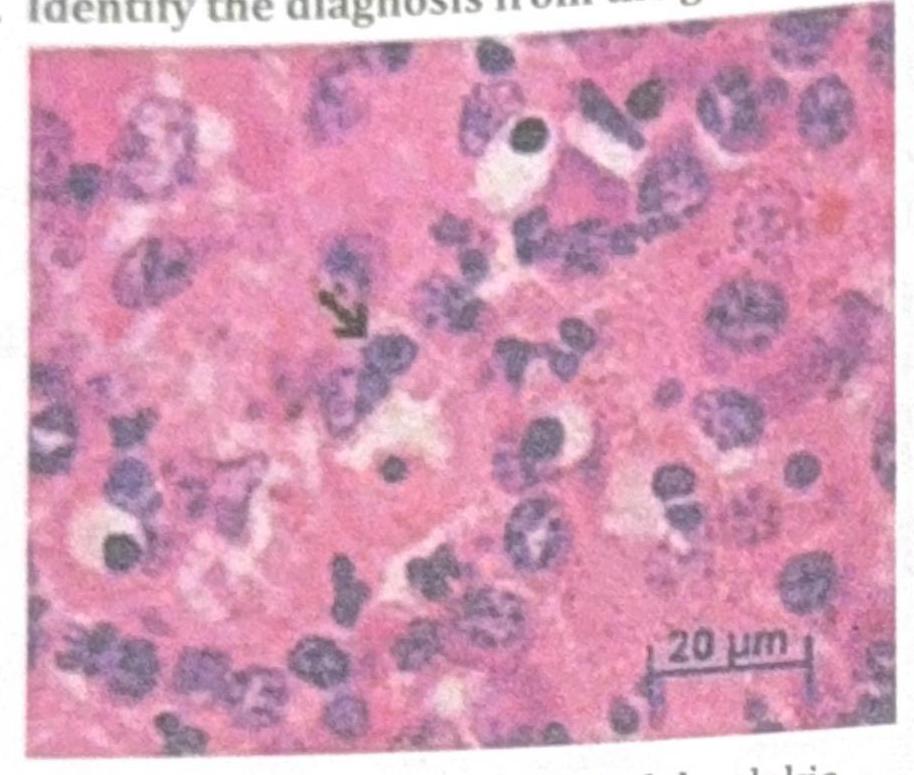
Q19
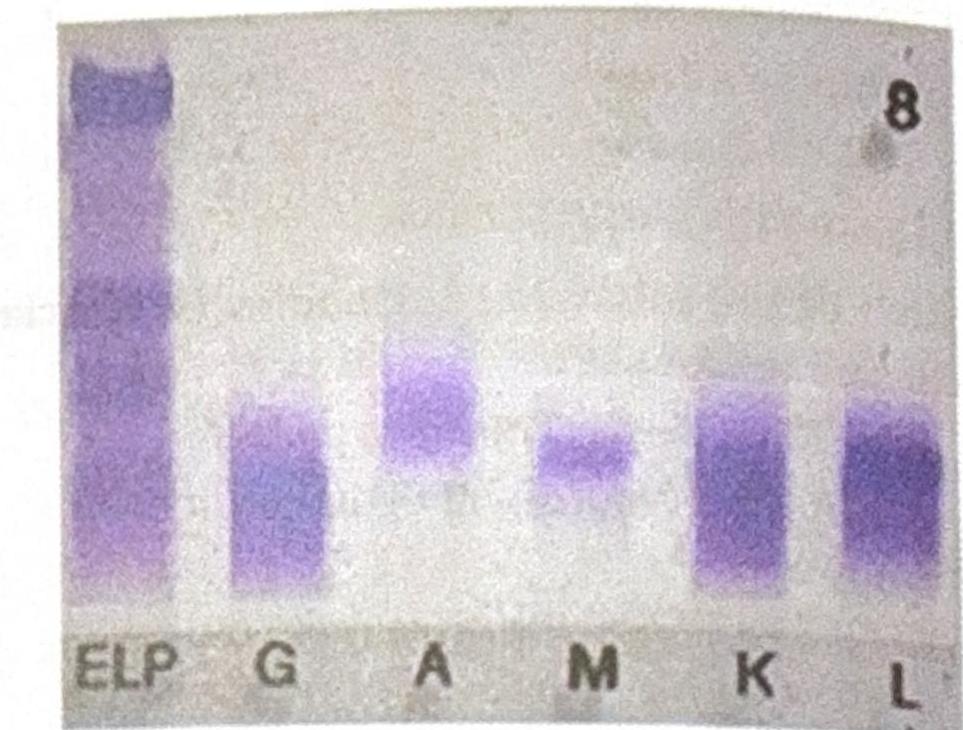
An elderly male patient presented with clinical symptoms and signs consistent with possible multiple myeloma. Electrophoresis shows an M spike, and immunofixation findings are shown below. Which of the following statements best corresponds to the findings?
Q20
Which of the following is an intracellular marker or deposition found in Alzheimer's disease?