NEET-PG 2024 — Pathology
16 Previous Year Questions with Answers & Explanations
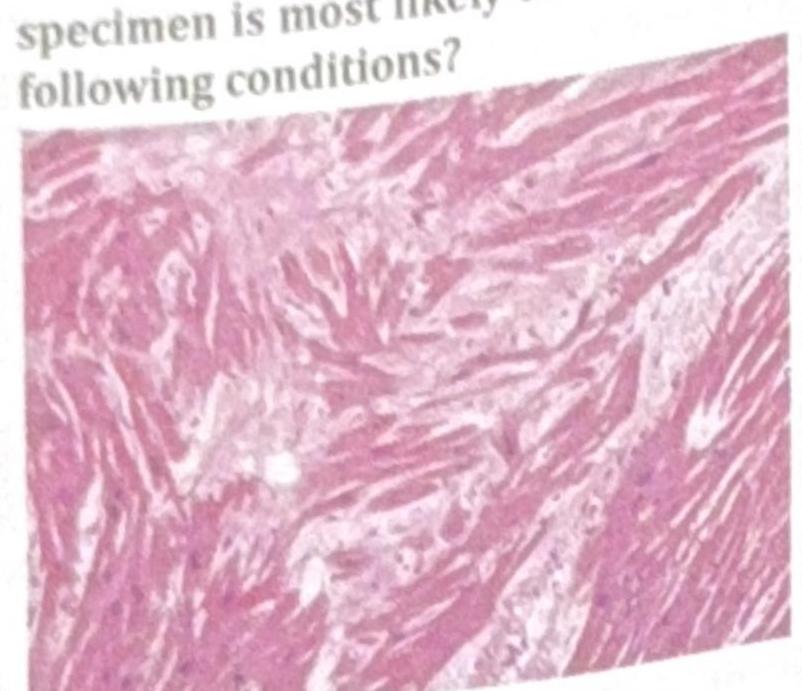
An athlete collapsed and expired while playing school basketball. Histology of the cardiac specimen is most likely to indicate which of the following conditions?
TTF-1 is a tumor marker for which of the following?
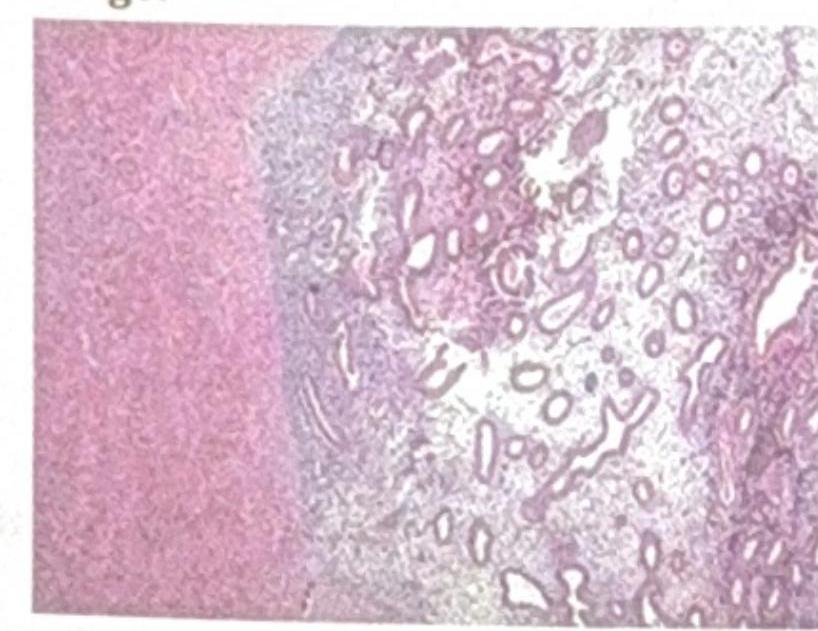
Identify the pathological condition shown in the image:
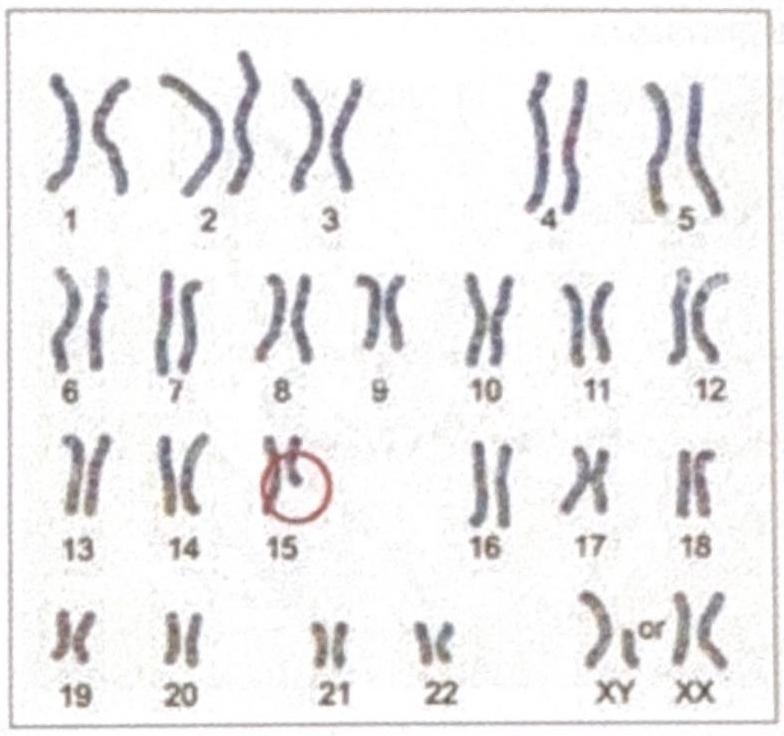
The diagrammatic representation of the karyotype of an individual indicates a specific genetic abnormality. What is the diagnosis?
Which PCR technique is best suited for identifying a syndrome with multiple causative agents?
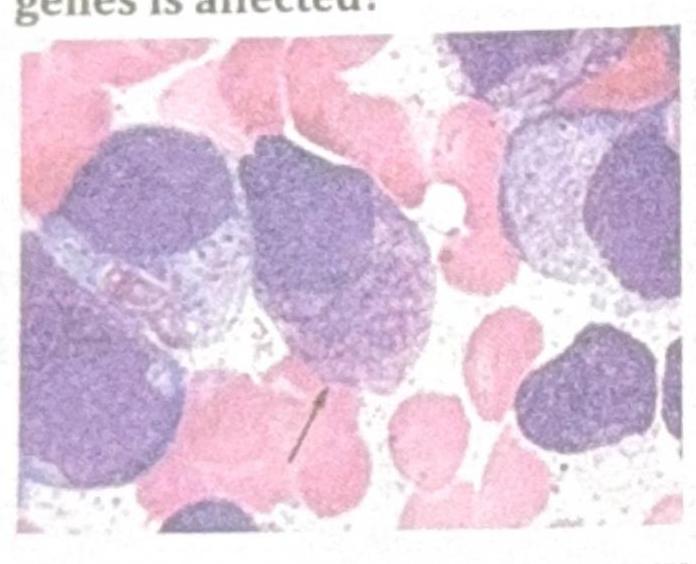
Identify the gene commonly involved in the condition shown in the image?
A patient has a cerebellar mass, renal tumor, and a family history of similar conditions. Which of the following mutations is most likely present in the family?
TTF-1 (Thyroid Transcription Factor-1) immunohistochemical marker is most commonly seen in which of the following?
A 23-year-old female with a height of 4 feet has a karyotype as shown in the image below. Which among the following indicates the correct etiology?
Identify the image and the disease it is associated with: 
NEET-PG 2024 - Pathology NEET-PG Practice Questions and MCQs
Question 1: An athlete collapsed and expired while playing school basketball. Histology of the cardiac specimen is most likely to indicate which of the following conditions?
- A. Dilated cardiomyopathy (DCM)
- B. Restrictive cardiomyopathy (RCM)
- C. Arrhythmogenic right ventricular dysplasia (ARVD)
- D. Hypertrophic cardiomyopathy (HCM) (Correct Answer)
Explanation: ***Hypertrophic cardiomyopathy (HCM)*** - The image shows **myocardial disarray and hypertrophy**, characterized by haphazardly arranged and abnormally branched cardiac muscle cells with large, irregular nuclei, which is a classic histologic finding in HCM [1]. - HCM is the most common cause of **sudden cardiac death in young athletes**, often during exertion, due to ventricular arrhythmias arising from the disarrayed myocardium [1]. *Dilated cardiomyopathy (DCM)* - Histology for DCM typically shows **myocyte atrophy**, thinning of the ventricular walls, and interstitial fibrosis, not the marked disarray and hypertrophy seen here [3]. - DCM leads to **progressive cardiac enlargement and systolic dysfunction**, and while it can cause sudden death, it is less common in athletes than HCM [4]. *Restrictive cardiomyopathy (RCM)* - RCM is characterized by **stiff, non-compliant ventricles** with impaired diastolic filling, often due to conditions like amyloidosis or sarcoidosis, showing interstitial infiltration or fibrosis. - The image does not show evidence of significant **interstitial infiltration or severe fibrosis** characteristic of RCM; instead, it highlights myocyte pathology. *Arrhythmogenic right ventricular dysplasia (ARVD)* - ARVD is characterized by the **replacement of right ventricular myocardium with fibrofatty tissue**, which would be evident histologically as fat and fibrous infiltration [2]. - While ARVD can cause sudden death in athletes, the displayed image primarily shows **myocyte hypertrophy and disarray**, not extensive fibrofatty replacement [2]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, pp. 577-578. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, pp. 576-577. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, p. 576. [4] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, pp. 559-560.
Question 2: TTF-1 is a tumor marker for which of the following?
- A. Adenocarcinoma
- B. Small cell carcinoma (Correct Answer)
- C. Thymoma
- D. Melanoma
Explanation: ***Small cell carcinoma*** - **Thyroid transcription factor 1 (TTF-1)** is a nuclear transcription protein expressed in lung and thyroid neoplasms - It is positive in **85-90% of small cell lung carcinomas**, making it a key immunohistochemical marker [1] - TTF-1 helps differentiate small cell carcinoma from other neuroendocrine tumors and extrapulmonary small cell carcinomas [1] *Adenocarcinoma* - TTF-1 is also **strongly positive in 75-80% of lung adenocarcinomas** - It is a primary marker for lung adenocarcinoma, often used with **Napsin A** and **Cytokeratin 7 (CK7)** *Thymoma* - Thymomas are neoplasms of the **thymus gland** and typically express **cytokeratins** but **not TTF-1** - Characteristic markers include **CD5**, **CD117**, and epithelial markers *Melanoma* - Melanomas are cancers of **melanocytes** and express melanocytic markers like **S-100**, **HMB-45**, **Melan-A**, and **SOX10** - **TTF-1** is not expressed in melanoma and helps exclude lung primary when evaluating metastatic disease **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 337-338.
Question 3: Identify the pathological condition shown in the image:
- A. Intramural fibroid
- B. Adenomyoma (Correct Answer)
- C. Endometriosis
- D. Myomatous polyp
Explanation: ***Adenomyoma*** - The image distinctly shows **endometrial glands and stroma** embedded within the **myometrium** (smooth muscle layer of the uterus), which is the hallmark of adenomyoma [1]. - This condition is essentially a localized form of **adenomyosis**, presenting as a mass [1]. *Intramural fibroid* - An intramural fibroid (leiomyoma) is a **benign tumor of smooth muscle cells**, typically showing a proliferation of uniform spindle cells with characteristic swirling patterns [2]. - It would lack the presence of **endometrial glands and stroma** within the lesion [2]. *Endometriosis* - Endometriosis involves the presence of **endometrial tissue outside the uterus**, such as on the ovaries, peritoneum, or bowel. - While it involves similar tissue, its location is **extrauterine**, whereas the image depicts a lesion within the uterine wall. *Myomatous polyp* - A myomatous polyp (or submucosal fibroid) is a **fibroid that protrudes into the uterine cavity**, often covered by endometrial tissue [2]. - The image does not show a polypoid growth extending into the cavity but rather glandular tissue directly within the muscle wall. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Female Genital Tract Disease, pp. 475-476. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Female Genital Tract, pp. 1024-1025.
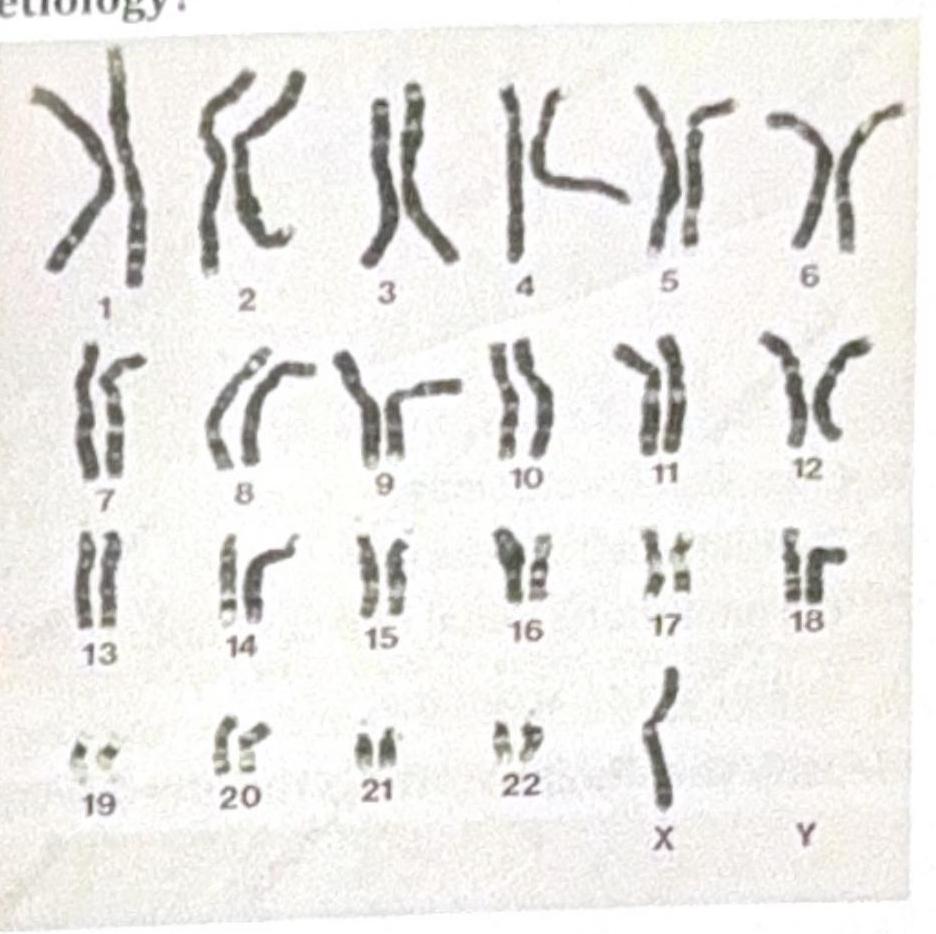
Question 4: The diagrammatic representation of the karyotype of an individual indicates a specific genetic abnormality. What is the diagnosis?
- A. Angelman syndrome
- B. Cri du Chat syndrome
- C. DiGeorge syndrome
- D. Prader-Willi syndrome (Correct Answer)
Explanation: ***Prader-Willi syndrome*** - The karyotype shows an abnormality on **chromosome 15**, which is consistent with Prader-Willi syndrome caused by **deletion of 15q11-q13** inherited from the **paternal** chromosome or **maternal uniparental disomy**. - While PWS deletions are typically **submicroscopic**, larger deletions can occasionally be visible on standard karyotyping, particularly when they represent **class I deletions** that are more extensive and involve additional chromosomal material beyond the typical PWS critical region. *Angelman syndrome* - Although Angelman syndrome also involves **chromosome 15q11-q13 deletion**, it results from **maternal** deletion or **paternal uniparental disomy**, and presents with distinctly different clinical features. - Clinical presentation includes **severe intellectual disability**, **ataxia**, **seizures**, **absent speech**, and **inappropriate laughter** (happy demeanor), which differs significantly from the PWS phenotype. *DiGeorge syndrome* - DiGeorge syndrome is caused by **deletion of chromosome 22q11.2**, not chromosome 15 as shown in the karyotype. - Clinical features include **cardiac defects** (conotruncal abnormalities), **thymic hypoplasia**, **parathyroid hypoplasia** (hypocalcemia), **cleft palate**, and characteristic facial features (CATCH-22 syndrome). *Cri du Chat syndrome* - This syndrome results from **deletion of chromosome 5p** (short arm of chromosome 5), not chromosome 15 as indicated in the karyotype. - Characteristic features include **high-pitched cry** resembling a cat's meow in infancy, **intellectual disability**, **microcephaly**, and **distinctive facial features**.
Question 5: Which PCR technique is best suited for identifying a syndrome with multiple causative agents?
- A. RT-PCR
- B. Multiplex PCR (Correct Answer)
- C. Nested PCR
- D. Conventional PCR
Explanation: ***Multiplex PCR*** - **Multiplex PCR** allows for the simultaneous amplification of **multiple DNA targets** in a single reaction, making it ideal for identifying syndromes with numerous potential causative agents. - This method uses **multiple primer pairs** in one reaction tube, each designed to amplify a specific target sequence, thus efficiently detecting various pathogens or genetic markers. *RT-PCR* - **Reverse Transcription PCR (RT-PCR)** is used to detect **RNA targets** by first converting RNA into cDNA, which is then amplified. - While useful for RNA viruses or gene expression studies, it is not primarily designed for simultaneous detection of multiple diverse causative agents in the same way as multiplex PCR. *Nested PCR* - **Nested PCR** uses two sets of primers in sequential reactions to **increase sensitivity and specificity** by reducing non-specific binding. - This technique is generally employed to detect very low copies of a specific target or to overcome issues with non-specific amplification, rather than for identifying multiple different agents concurrently. *Conventional PCR* - **Conventional PCR** amplifies a **single specific DNA target** using one pair of primers per reaction. [1] - It requires separate reactions for each potential causative agent, making it inefficient and labor-intensive when testing for a syndrome with multiple etiologies. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 56-57.
Question 6: Identify the gene commonly involved in the condition shown in the image?
- A. RAS
- B. RET
- C. BRAF V600E (Correct Answer)
- D. P53
Explanation: ***BRAF V600E*** - The image displays cells with **Langerhans cell morphology**, including folded nuclei and abundant pale cytoplasm, which are characteristic of **Langerhans cell histiocytosis (LCH)** [1]. - The **BRAF V600E mutation** is the most common genetic alteration found in LCH, present in about 50-60% of cases and activating the MAPK pathway [1]. *RAS* - **RAS mutations** are frequently seen in various cancers, including colorectal adenocarcinoma, pancreatic adenocarcinoma, and non-small cell lung cancer. - While RAS pathway activation can occur in LCH, a direct RAS mutation is not the most common genetic driver; rather, downstream effectors like BRAF V600E are more prominent [1]. *RET* - **RET mutations** are primarily associated with **medullary thyroid carcinoma** (in both sporadic and inherited forms like MEN 2A and MEN 2B) and can also be found in certain types of lung cancer. - They are not a characteristic genetic alteration for Langerhans cell histiocytosis. *P53* - The **TP53 gene** encodes the tumor suppressor protein p53, and mutations in this gene are among the most frequent genetic alterations across a wide spectrum of human cancers. - Although p53 plays a critical role in cell cycle regulation and apoptosis, it is not a primary or common driver mutation specifically associated with Langerhans cell histiocytosis [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 629-630.
Question 7: A patient has a cerebellar mass, renal tumor, and a family history of similar conditions. Which of the following mutations is most likely present in the family?
- A. VHL (Correct Answer)
- B. Neurofibromatosis (NF1)
- C. Tuberous Sclerosis Complex (TSC)
- D. Li-Fraumeni syndrome
Explanation: ***VHL*** - **Von Hippel-Lindau (VHL) disease** is an inherited disorder characterized by the development of tumors and cysts in various parts of the body, including **hemangioblastomas** in the cerebellum and retina, **renal cell carcinomas**, and pheochromocytomas [1]. - The combination of a **cerebellar mass**, renal tumor, and a family history strongly points to VHL disease, which is caused by a germline mutation in the **VHL tumor suppressor gene** [1]. *Neurofibromatosis (NF1)* - **Neurofibromatosis type 1 (NF1)** typically presents with multiple neurofibromas, **café-au-lait spots**, optic pathway gliomas, and Lisch nodules in the iris. - While NF1 can cause tumors, the specific combination of a cerebellar mass and renal tumor is not typical of NF1, and the characteristic skin findings are not mentioned. *Tuberous Sclerosis Complex (TSC)* - **Tuberous Sclerosis Complex (TSC)** is characterized by the growth of benign tumors in the brain (e.g., **subependymal giant cell astrocytomas**), kidneys (e.g., **angiomyolipomas**), heart, lungs, and skin (e.g., facial angiofibromas) [2]. - While TSC can involve brain and kidney tumors, the typical brain tumors are different (astrocytomas vs. hemangioblastomas), and hemangioblastomas are not a common feature of TSC [2]. *Li-Fraumeni syndrome* - **Li-Fraumeni syndrome** is a rare inherited cancer predisposition syndrome characterized by a high risk of developing various cancers, including **sarcomas**, breast cancer, brain tumors (often astrocytomas or medulloblastomas), and adrenocortical carcinoma. - While brain tumors are part of Li-Fraumeni syndrome, renal cell carcinoma is not a primary feature, and the classic cerebellar hemangioblastoma is not typical for this syndrome. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Manifestations Of Central And Peripheral Nervous System Disease, pp. 724-727. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Central Nervous System, pp. 1318-1319.
Question 8: TTF-1 (Thyroid Transcription Factor-1) immunohistochemical marker is most commonly seen in which of the following?
- A. Squamous Cell Carcinoma (SCC)
- B. Lung adenocarcinoma (Correct Answer)
- C. Large cell lung cancer
- D. Papillary thyroid carcinoma
Explanation: ***Lung adenocarcinoma*** - **TTF-1 (Thyroid Transcription Factor-1)** is a nuclear transcription factor that is highly expressed in adenocarcinomas of the lung. Positivity for TTF-1 is a key marker used in the diagnosis of primary lung adenocarcinoma, distinguishing it from other lung cancers and metastatic tumors. - While TTF-1 can also be positive in thyroid follicular and papillary carcinomas, its strong association with **lung adenocarcinoma** makes it a crucial diagnostic marker in this context, especially when differentiating between primary lung tumors and metastases or other lung cancer types. *Squamous Cell Carcinoma (SCC)* - **Squamous cell carcinoma of the lung** is generally **negative for TTF-1**. It typically expresses markers like p40 and CK5/6. - TTF-1 has very low sensitivity and specificity for squamous cell carcinoma, making it a poor choice for identifying this type of lung cancer. *Large cell lung cancer* - **Large cell lung carcinoma** is a diagnosis of exclusion and is typically **negative for TTF-1**, as well as other specific markers for adenocarcinoma or squamous cell carcinoma. - This type of cancer is characterized by large, anaplastic cells that lack features of other specific lung cancer types when viewed under a microscope. *Papillary thyroid carcinoma* - While **papillary thyroid carcinoma** is also **TTF-1 positive**, the question asks for the most common context in which TTF-1 is seen, and TTF-1 is a highly valuable marker for confirming a lung primary in the setting of lung masses. - TTF-1's utility in lung cancer diagnostics is particularly significant for differentiating primary lung adenocarcinomas from metastatic tumors and other lung cancer subtypes.
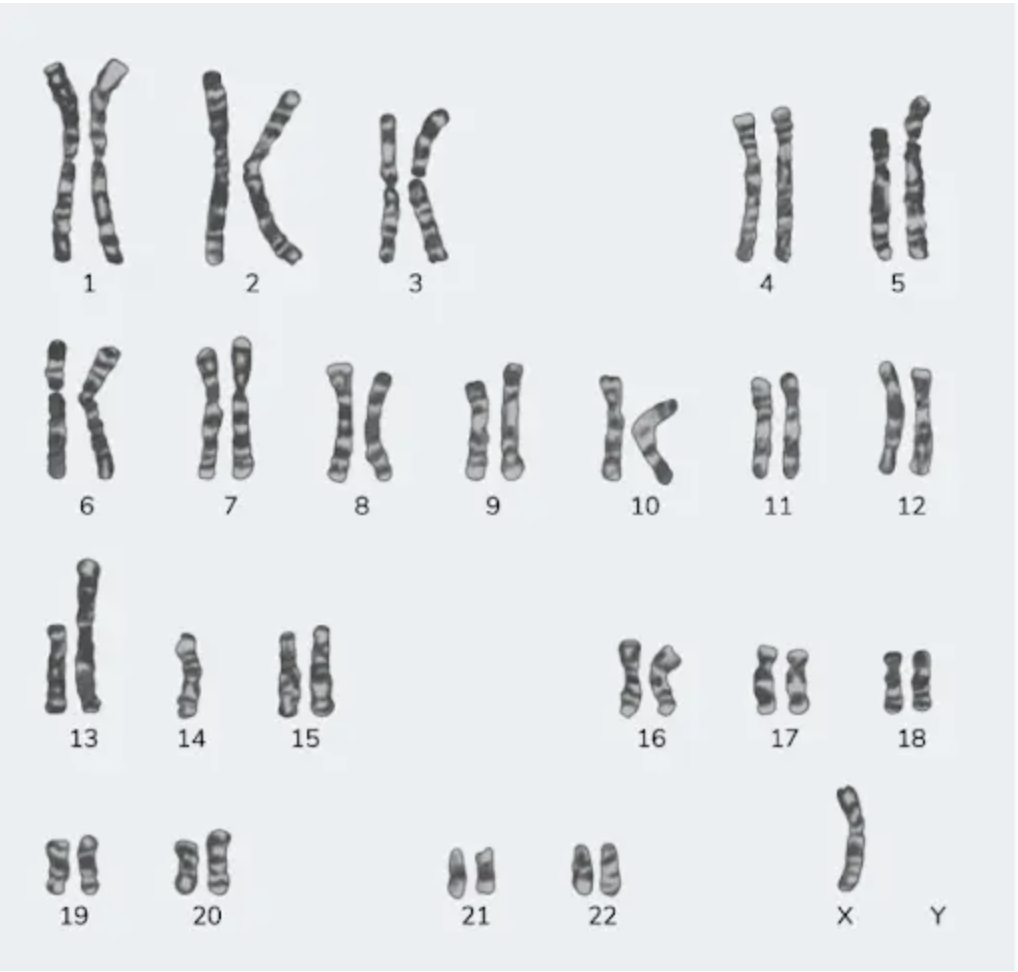
Question 9: A 23-year-old female with a height of 4 feet has a karyotype as shown in the image below. Which among the following indicates the correct etiology?
- A. Turner syndrome (Correct Answer)
- B. Klinefelter's syndrome
- C. Down syndrome
- D. Edward's syndrome
Explanation: **Turner syndrome** - The **karyotype shows 45,X**, meaning there is only one X chromosome and no second sex chromosome (Y or another X). This absence of a full second sex chromosome is the defining genetic characteristic of **Turner syndrome** [1]. - The clinical presentation of a **23-year-old female with a height of 4 feet (short stature)** is a classic sign of Turner syndrome, which results from the partial or complete monosomy of the X chromosome. Short stature in these patients is specifically linked to the haploinsufficiency of the SHOX gene [1]. *Klinefelter's syndrome* - This syndrome is characterized by the presence of an **extra X chromosome in males**, leading to a karyotype typically 47,XXY [2]. - While individuals with Klinefelter's syndrome may also have a variety of physical and developmental challenges, the patient's biological sex (female) and the specific karyotype shown **(45,X)** do not align with this condition. *Down syndrome* - Down syndrome is caused by a **trisomy of chromosome 21**, meaning there are three copies of chromosome 21 instead of the usual two [2]. - The provided karyotype clearly shows **two copies of chromosome 21** and a sex chromosome abnormality (45,X), making Down syndrome an incorrect diagnosis [1]. *Edward's syndrome* - Edward's syndrome is characterized by a **trisomy of chromosome 18**, meaning there are three copies of chromosome 18 [1]. - The presented karyotype shows **two copies of chromosome 18** and an abnormality in the sex chromosomes, ruling out Edward's syndrome. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, pp. 171-177. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 92-93.
Question 10: Identify the image and the disease it is associated with: 
- A. Gaucher's disease (Correct Answer)
- B. Tay-Sachs disease
- C. Sandhoff's disease
- D. Fabry's disease
Explanation: ***Gaucher's disease*** - The image shows **Gaucher cells** - characteristic lipid-laden macrophages with a distinctive **"crumpled tissue paper" or "wrinkled silk" cytoplasmic appearance** and eccentric nuclei [1] - These cells are pathognomonic for **Gaucher's disease**, an **autosomal recessive lysosomal storage disorder** caused by **glucocerebrosidase deficiency** [1] - Accumulation of **glucocerebroside** in macrophages creates the characteristic morphology seen in bone marrow, spleen, and liver [1] - Caused by mutations in the *GBA* gene on chromosome 1 [1] *Tay-Sachs disease* - Autosomal recessive disorder caused by **hexosaminidase A deficiency** leading to **GM2 ganglioside accumulation** [2] - Characteristic findings include **cherry-red spot on macula** and neuronal ballooning, not the macrophage changes seen in this image [2] - Does not produce Gaucher cells *Sandhoff's disease* - Caused by deficiency of both **hexosaminidase A and B** due to *HEXB* gene mutations - Similar to Tay-Sachs with GM2 ganglioside accumulation affecting neurons - Does not produce the characteristic macrophage morphology shown in the image *Fabry's disease* - **X-linked recessive** disorder caused by **alpha-galactosidase A deficiency** - Accumulation of **globotriaosylceramide** in vascular endothelial cells - Histology may show lipid deposits in vessels and kidney, not the distinctive Gaucher cells seen here **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, pp. 162-163. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, p. 161.