All (378)Anatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q301
Which of the following phases are directly involved in the recovery phase of the disaster cycle?
Q302
What does JSSK stand for?
Q303
Identify the logo?
Q304
The formula with the numerator as maternal deaths and the denominator as women of reproductive age is used to calculate which of the following?
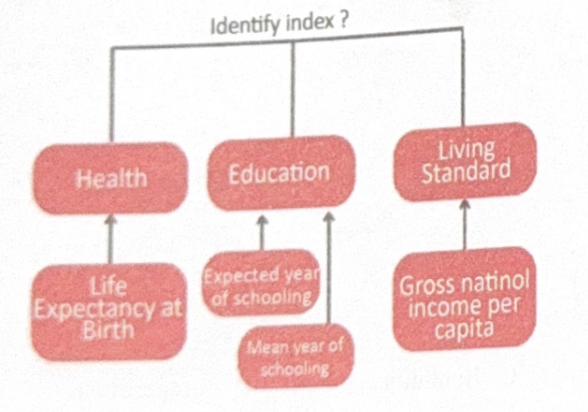
Q305
Identify the index?
Q306
Which of the following is not a component of Physical Quality of Life Index (PQLI)?
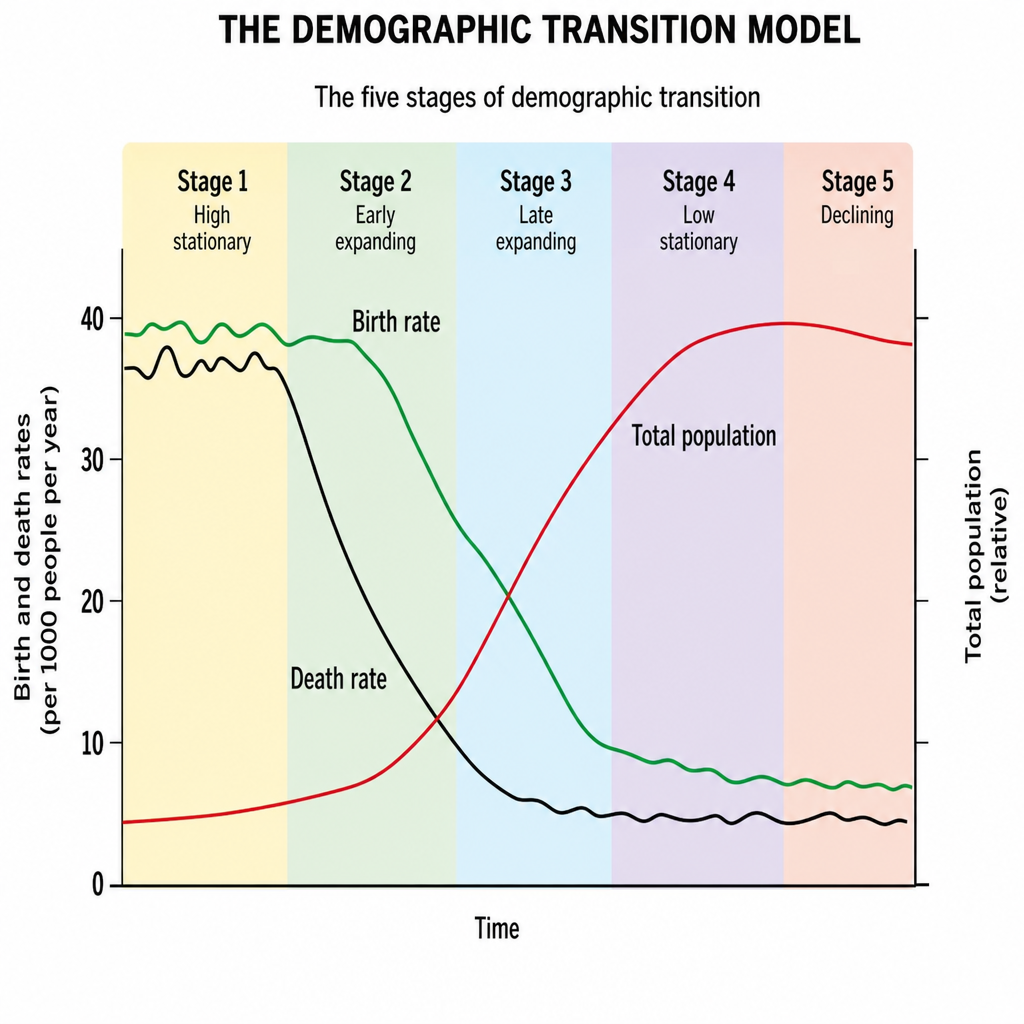
Q307
The Black Line in the demographic cycle represents:
Q308
Given the following data: 500 live births and 9 deaths within the first 7 days, calculate the early neonatal mortality rate.