All (378)Anatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q271
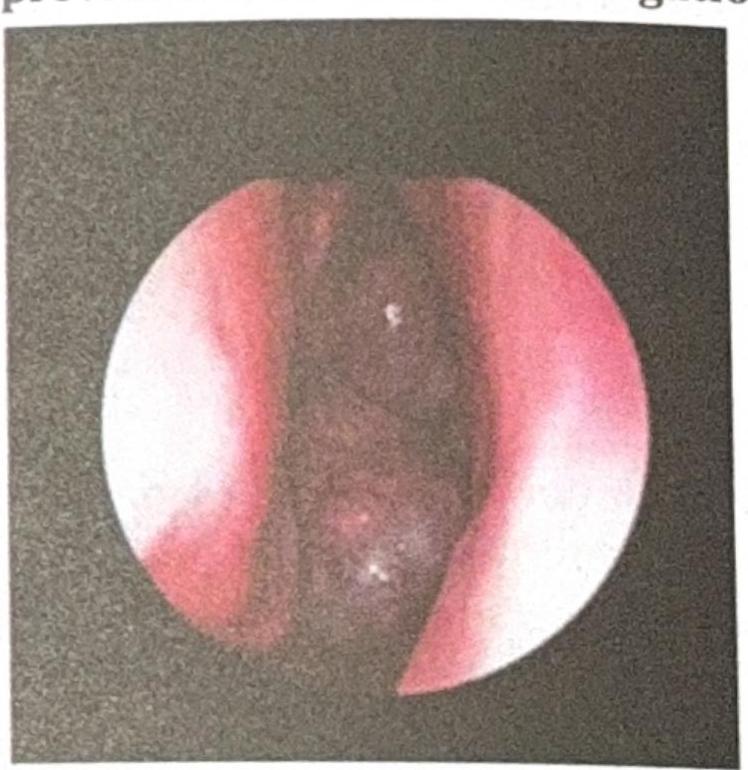
A 14-year-old child with a history of recurrent nasal bleeding has the endoscopic view provided. What is the investigation of choice?
Q272
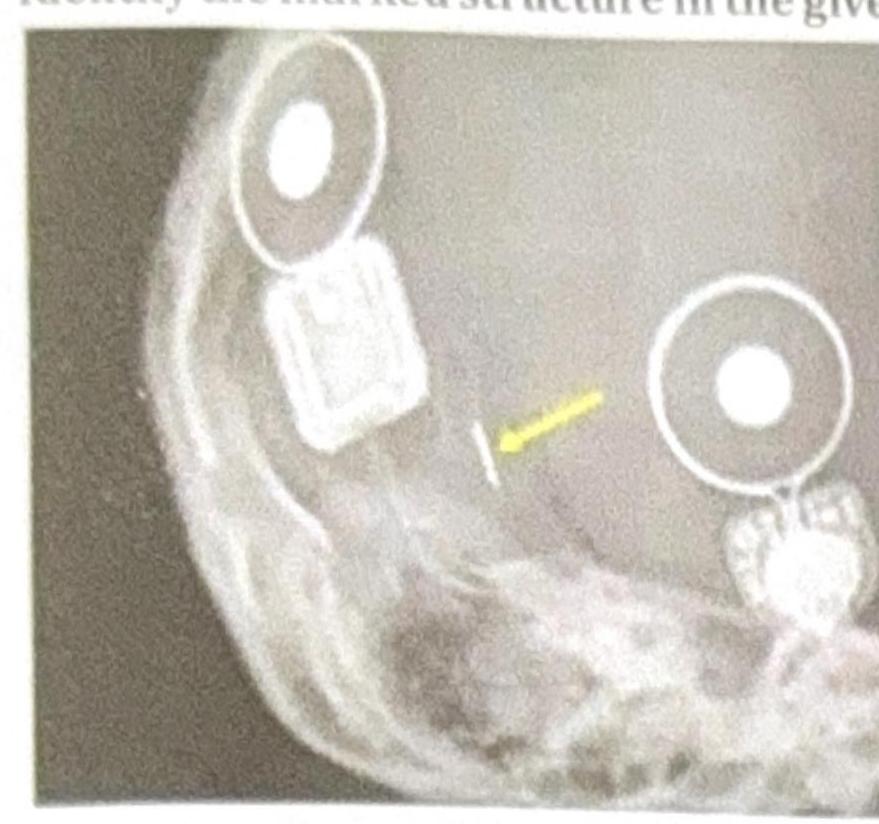
Identify the marked structure in the given image.
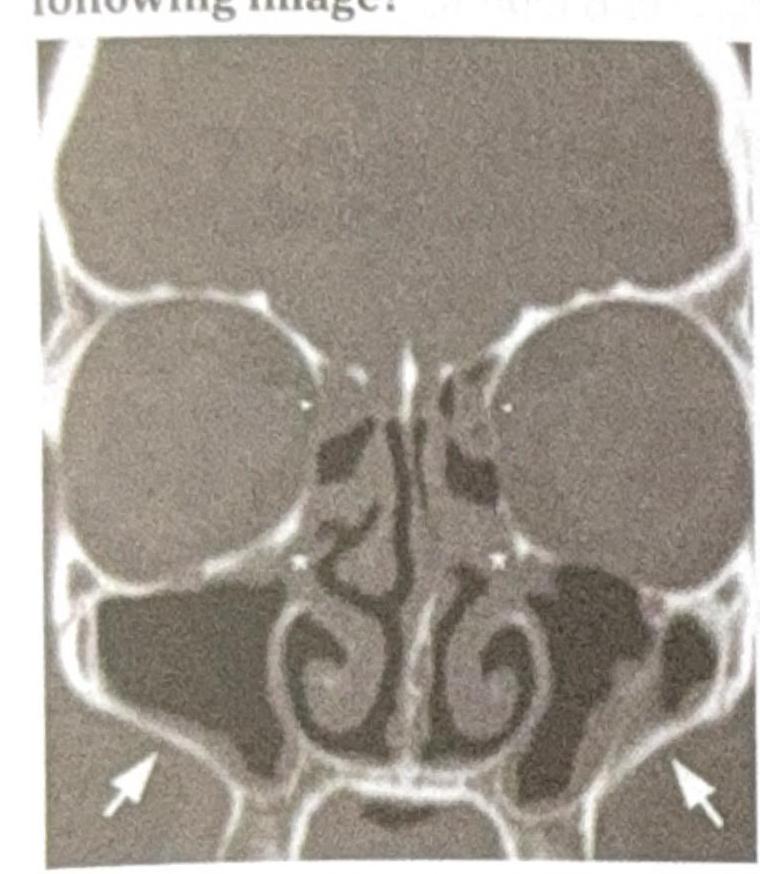
Q273
Which sinus drainage is impaired in the following image?
Q274
A female patient's pure tone audiometry (PTA) findings show the presence of a Carhart's notch. Which of the following specific clinical signs can be seen in this patient?