All (378)Anatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q241
A patient has a cerebellar mass, renal tumor, and a family history of similar conditions. Which of the following mutations is most likely present in the family?
Q242
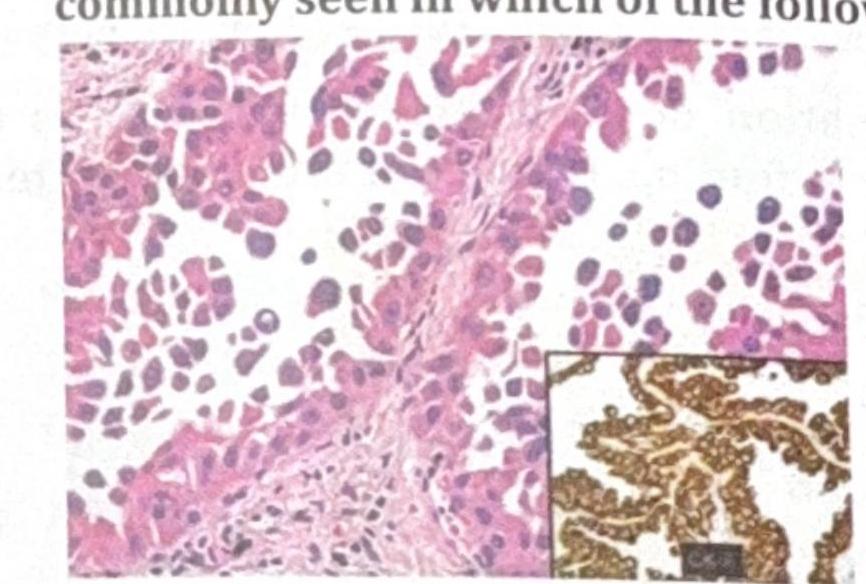
TTF-1 (Thyroid Transcription Factor-1) immunohistochemical marker is most commonly seen in which of the following?
Q243
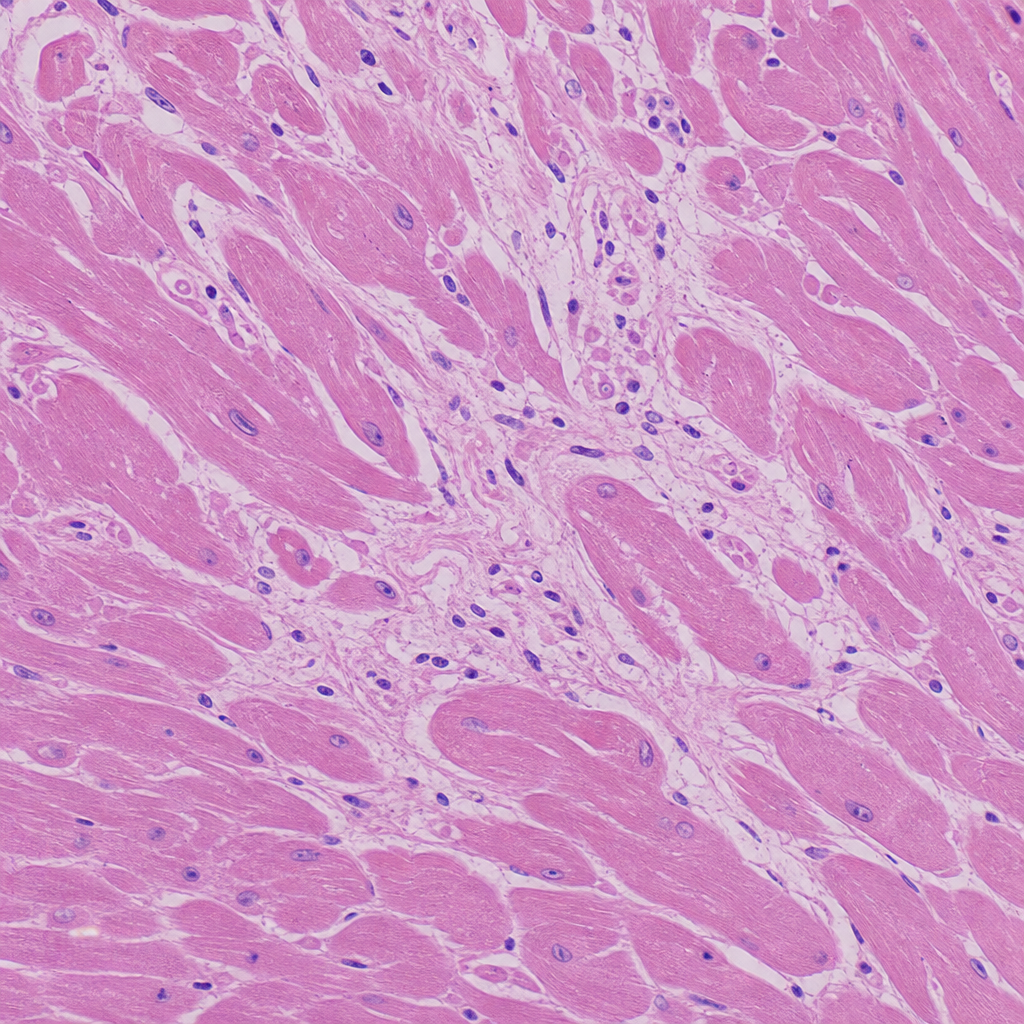
A 30-year-old football player presented to the emergency department with sudden cardiac arrest/collapse. Based on the histological image provided, what is the most likely cause of his death?
Q244
The skin biopsy shown below is most consistent with which of the following conditions? 
Q245
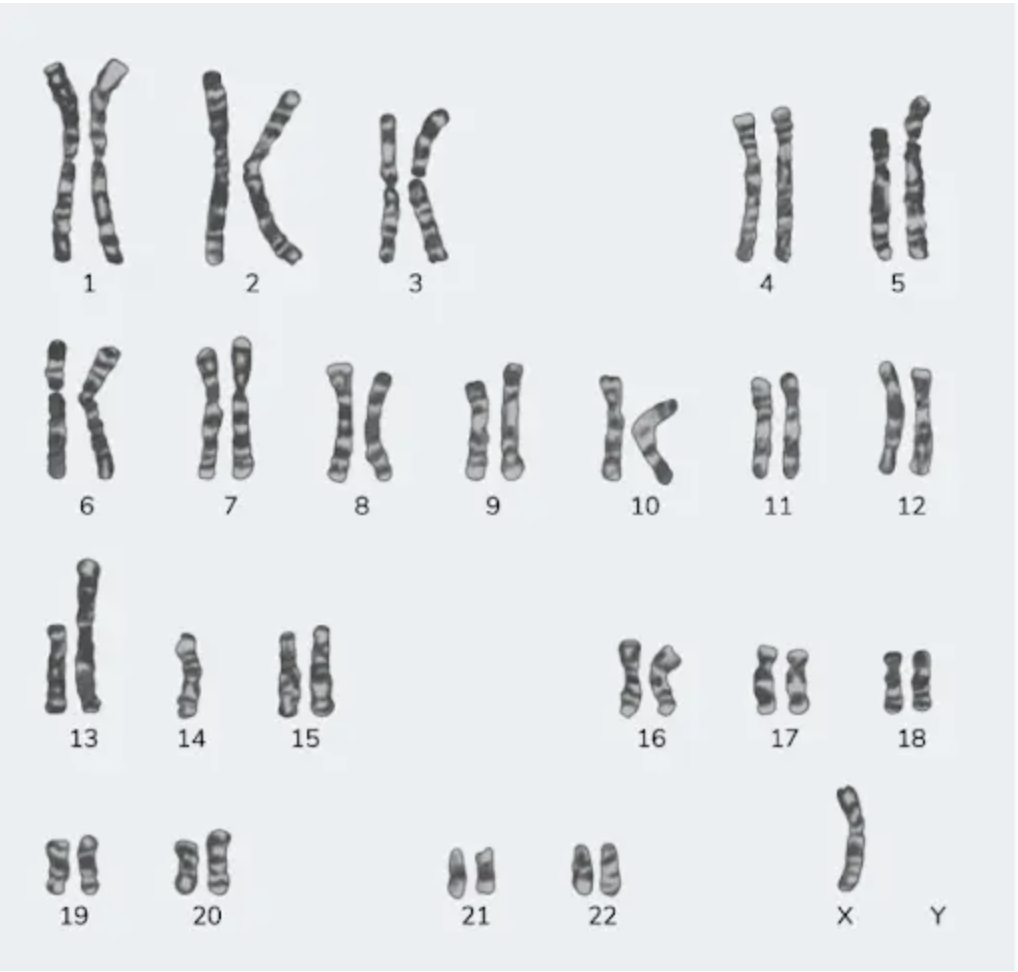
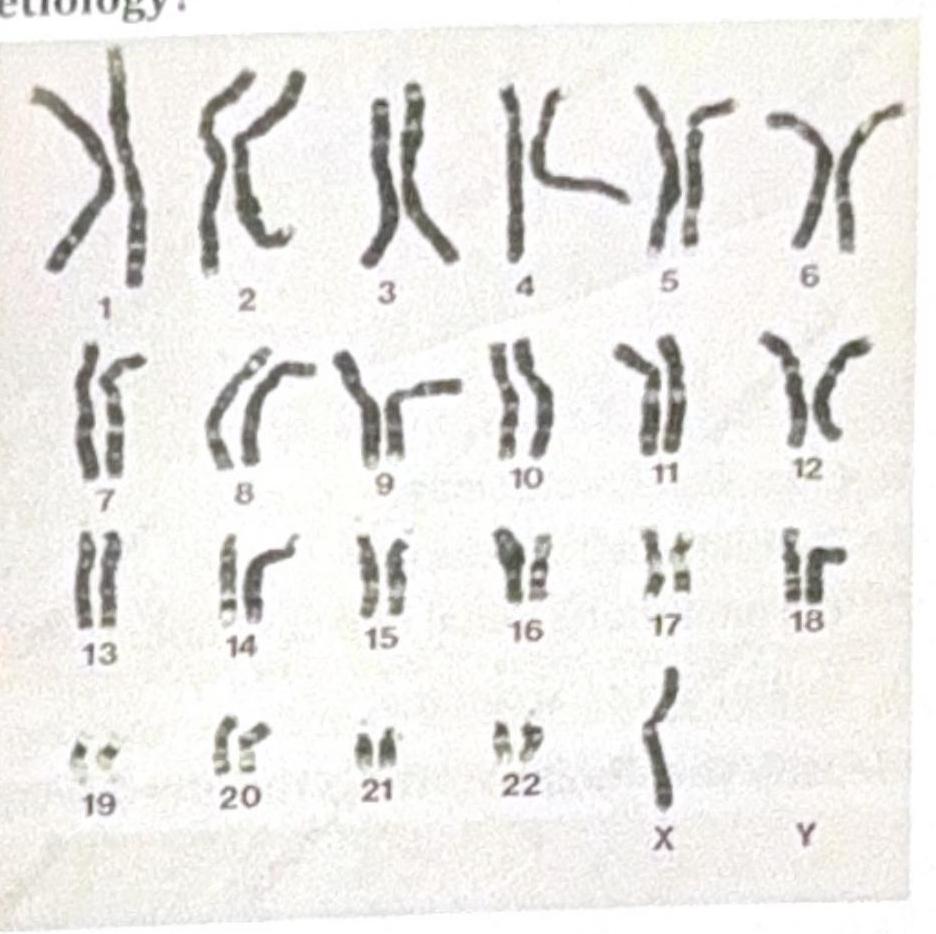
A 23-year-old female with a height of 4 feet has a karyotype as shown in the image below. Which among the following indicates the correct etiology?
Q246
The histopathology image shown is characteristic of which of the following diseases? 
Q247
A male patient is not responding to oxygen therapy and has been diagnosed with ARDS (Acute Respiratory Distress Syndrome). What is the role of IL-8 in ARDS?