All (378)Anatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q191
Aprepitant is a drug used in the treatment of some cases of chemotherapy-induced nausea and vomiting. What is the mechanism of action of this drug?
Q192
Which of the following is an inclusion criterion for the shorter bedaquiline regimen in the treatment of tuberculosis?
Q193
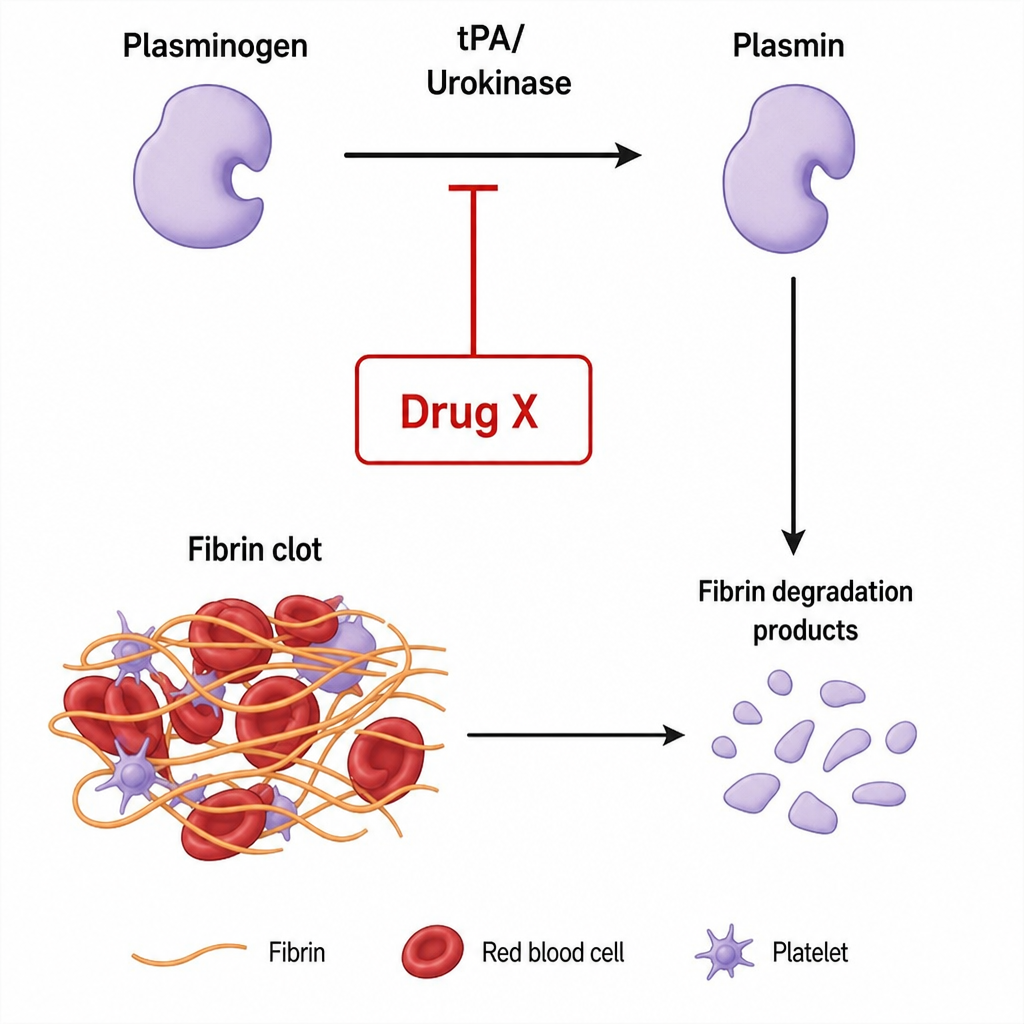
Which of the following is represented in the below figure by drug X?
Q194
A patient presents with hypertension and has a history of renal stones, along with several episodes of renal colic. Which diuretic is the most appropriate to use?
Q195
Which of the following is the most appropriate treatment for an overactive bladder in a patient with dementia?
Q196
Which of the following statements regarding the patch shown in the figure is correct?

Q197
Lidocaine is used in a loading dose for the treatment of arrhythmias. The loading dose of this drug depends upon which of the following factors?
Q198
A person was taking an antihypertensive drug and continued taking it despite developing constipation, dry mouth, and dizziness. He was taking it regularly but forgot to take it during a trip abroad and has now developed a hypertensive emergency. Which antihypertensive was he likely taking?