All (378)Anatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q11
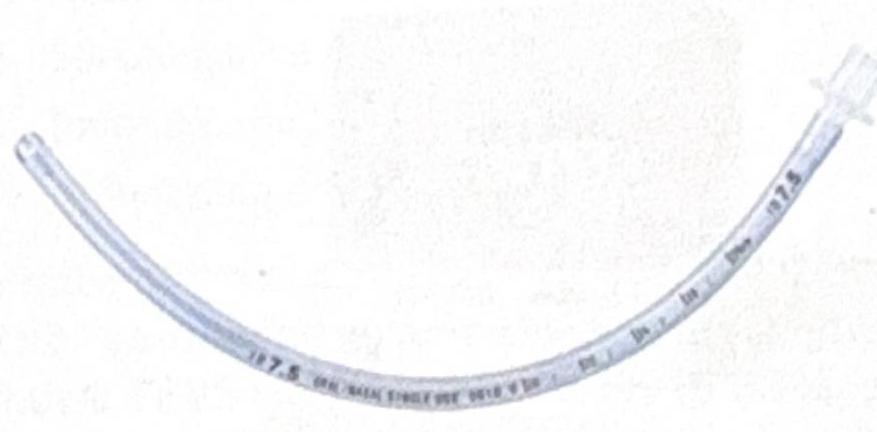
Identify the instrument shown in the image:
Q12
What is the purpose of Positive End-Expiratory Pressure (PEEP)?
Q13
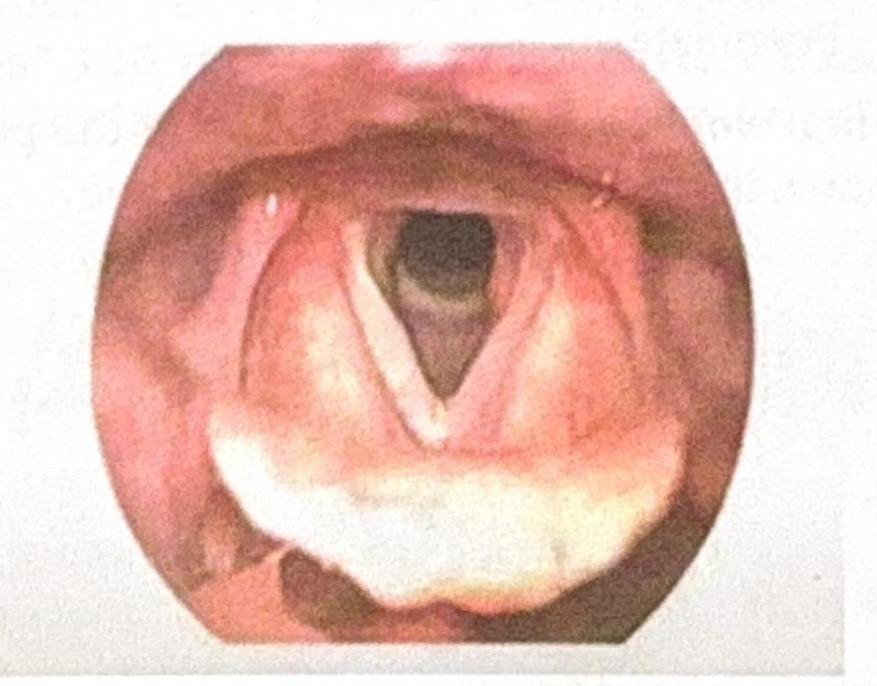
What is the staging system used for the condition seen in the patient after a history of intubation, as shown in the image?
Q14
What is the name of the nerve block technique shown in the image?
Q15
A patient presented with rigidity, tremors, and trismus after being administered an anesthetic agent. Which anesthetic agent is most likely to have been administered?
Q16
In which clinical scenario would you find a patient requiring the vital signs assessment technique shown in the image?