All (378)Anatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q181
A woman presents with a chronic history of fever and lower limb swelling. The microscopic image of a parasite in her blood smear is shown. Identify the pathogen responsible for her condition.

Q182
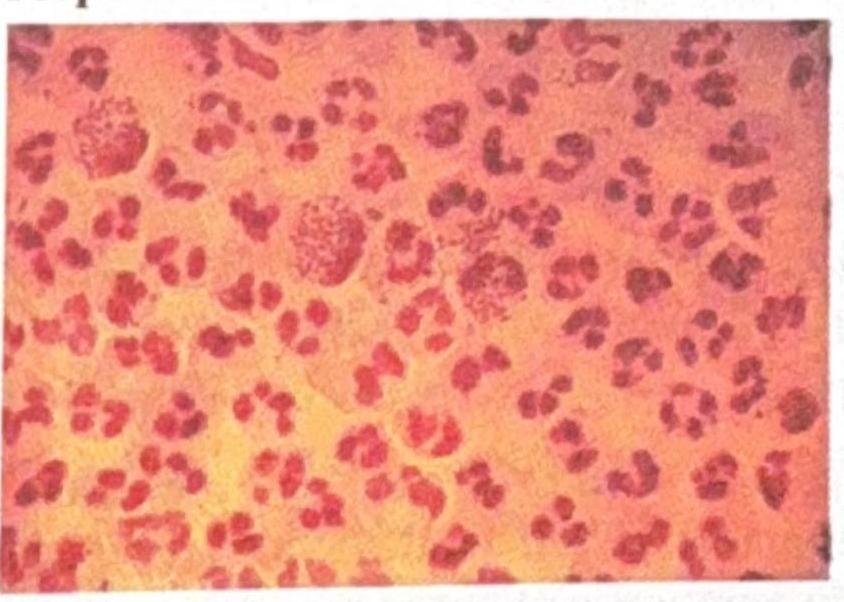
A man presents with dysuria and urethral discharge after a history of unprotected sex. The Gram stain of his discharge is shown. What is the best culture medium for isolating the organism responsible?
Q183
A young boy who used to wash his contact lenses in tap water or with unhygienic lens fluid developed keratitis. Microscopy revealed an organism with spiked or star-shaped structures. Identify the correct organism responsible.
Q184
A patient in the ICU with a central venous catheter (CVC) develops an infection. Microscopy reveals ovoid budding yeast cells. What is the most likely organism?
Q185
A farmer presents with a subcutaneous wound on his foot with discharge. Microscopy of a white granule from the wound shows Gram-positive filamentous rods. What is the most likely organism?