All (378)Anatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q111
The X-ray shows plating done for a fracture. How does this fracture heal?

Q112
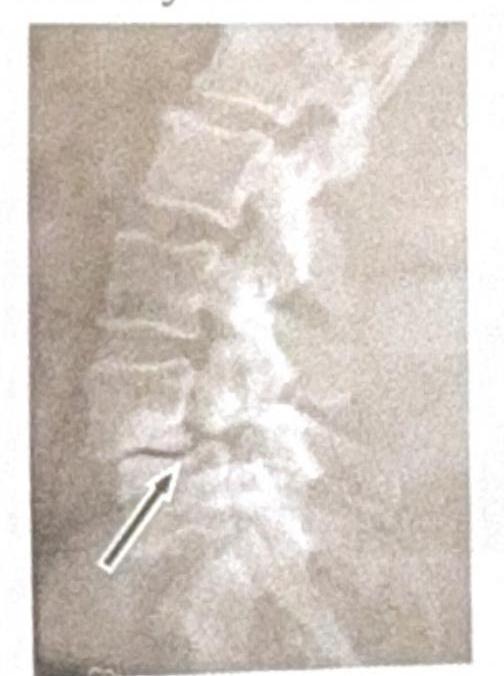
Identify the condition shown in the image:
Q113
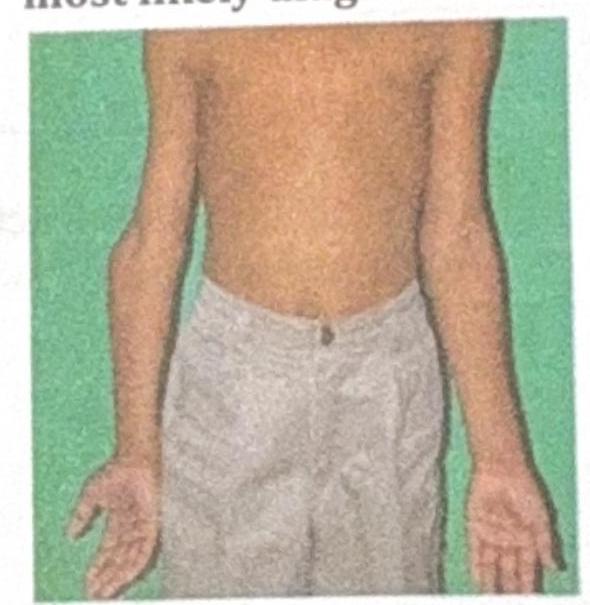
A 10-year-old boy presents with the physical findings shown in the image, characterized by inward angulation of the elbows. What is the most likely diagnosis?
Q114
Fracture at which site affects the longitudinal growth of a bone?