NEET-PG 2024 — Orthopaedics
10 Previous Year Questions with Answers & Explanations
A 35-year-old male presents to the emergency department following a high-speed motor vehicle accident. He complains of severe lower back pain but denies any loss of consciousness or abdominal pain. A lateral X-ray of the lumbar spine is obtained, as shown in the image. The image reveals a horizontal fracture through the vertebral body, extending through the posterior elements. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?

The image shows a pediatric fracture involving the growth plate. Which classification system and stage best describes this fracture?

Identify the implant shown in the image:

A patient presents with a 5th metatarsal fracture. How many days would he/she need to wear a cast?

A football player experienced a twist in the ankle and knee. Clinically, no bone injury was appreciated. The examiner is performing the test shown in the image. Which test is this?
The X-ray shows plating done for a fracture. How does this fracture heal?

Identify the condition shown in the image:
A 10-year-old boy presents with the physical findings shown in the image, characterized by inward angulation of the elbows. What is the most likely diagnosis?
Fracture at which site affects the longitudinal growth of a bone?
An 18-year-old boy presents with tenderness, warmth over the bone, and fever, ESR and CRP levels. The radiograph is shown below. What is the most likely diagnosis?
NEET-PG 2024 - Orthopaedics NEET-PG Practice Questions and MCQs
Question 1: A 35-year-old male presents to the emergency department following a high-speed motor vehicle accident. He complains of severe lower back pain but denies any loss of consciousness or abdominal pain. A lateral X-ray of the lumbar spine is obtained, as shown in the image. The image reveals a horizontal fracture through the vertebral body, extending through the posterior elements. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?
- A. Burst fracture
- B. Compression fracture
- C. Chance fracture (Correct Answer)
- D. Spondylolisthesis
Explanation: ***Chance fracture*** - A **chance fracture** is characterized by a **horizontal fracture** through the entire vertebral body and posterior elements, including the neural arch, typically caused by a **flexion-distraction mechanism** in accidents like those involving seatbelts (lap belt only), consistent with the high-speed motor vehicle accident scenario. - The image distinctly shows a fracture line traversing the vertebral body and extending into the posterior elements, which is the hallmark of this type of injury. *Burst fracture* - A **burst fracture** involves a comminuted fracture of the vertebral body with **retropulsion of bone fragments** into the spinal canal due to axial loading, which is not clearly depicted here. - While it can result from high-impact trauma, the characteristic horizontal disruption of both anterior and posterior segments points away from a solely compressive mechanism. *Compression fracture* - A **compression fracture** primarily involves the **anterior wedging** or collapse of the vertebral body, resulting from only axial compression forces without significant involvement of the posterior elements. - The presented image shows a fracture extending through the posterior elements, which is not typical for a simple compression fracture. *Spondylolisthesis* - **Spondylolisthesis** is the **anterior slippage of one vertebral body over another**, often due to pars interarticularis defects (spondylolysis) or degenerative changes. - This condition involves vertebral displacement, not a fresh fracture line across the body and posterior elements as seen in the image.
Question 2: The image shows a pediatric fracture involving the growth plate. Which classification system and stage best describes this fracture?
- A. Gartland 3
- B. Salter Harris 3 (Correct Answer)
- C. Gartland 2
- D. Salter Harris 2
Explanation: ***Salter Harris 3*** - The image shows a **fracture extending from the epiphyseal surface down through the growth plate (physis) and exiting through the epiphysis** into the joint. This configuration is characteristic of a Salter-Harris type III fracture. - Salter-Harris Type III fractures disrupt the **articular cartilage** and can have a poorer prognosis due to potential joint incongruity and growth disturbance if not properly reduced. *Gartland 3* - The **Gartland classification** is specifically used for **supracondylar fractures of the humerus** in children, which is a different type of fracture involving the distal humerus metaphysis, not typically the growth plate itself in this manner. - Gartland type 3 refers to a **completely displaced supracondylar fracture** with no cortical contact, involving the metaphysis proximal to the growth plate. *Gartland 2* - **Gartland type 2** describes a **displaced supracondylar fracture** with an intact posterior cortex, also referring to a fracture of the distal humerus metaphysis, not a trans-growth plate fracture. - This classification is not applicable to the image which clearly depicts a fracture involving the epiphysis and physis. *Salter Harris 2* - A **Salter-Harris type II fracture** involves the **physis and extends into the metaphysis**, creating a triangular fragment known as the "Thurston Holland sign." - In the provided image, the fracture line clearly extends into the **epiphysis**, not just the metaphysis, distinguishing it from a Salter-Harris type II.
Question 3: Identify the implant shown in the image:
- A. Dynamic hip screw (Correct Answer)
- B. Cannulated hip screw
- C. Condylar hip screw
- D. Intramedullary nail
Explanation: ***Dynamic hip screw*** - The image shows a **lag screw** inserted into the femoral neck and head, which slides within a **side plate** attached to the femoral shaft with cortical screws. - This construct allows for controlled **dynamic collapse** and impaction at the fracture site, promoting healing and providing stable fixation for **extracapsular hip fractures**. *Cannulated hip screw* - Cannulated screws are typically used in a **parallel configuration** or as a single large screw for hip fractures, particularly **femoral neck fractures**. - They do not feature a **side plate** that extends down the femoral shaft for additional fixation. *Condylar hip screw* - A condylar hip screw (DCS) is used for **distal femur fractures**, often extending into the **condyles**. - It involves a different angulation and design compared to the proximal femoral implant seen, which is fixed to the femoral shaft. *Intramedullary nail* - An intramedullary nail is inserted into the **medullary canal** of the bone, running through its center. - While some hip nails (e.g., trochanteric nails) have a cephalic screw component, they primarily stabilize the shaft from within, unlike the **extracortical side plate** seen here.
Question 4: A patient presents with a 5th metatarsal fracture. How many days would he/she need to wear a cast?
- A. 6-8 weeks (Correct Answer)
- B. 2-3 weeks
- C. 16-20 weeks
- D. 3-5 weeks
Explanation: ***6-8 weeks*** - For most **5th metatarsal fractures**, especially **Jones fractures** or more significant avulsion fractures, **non-weight-bearing** immobilization in a cast, boot, or splint is typically required for **6 to 8 weeks** to allow for proper bone healing. - The **poor vascular supply** to the metaphyseal-diaphyseal junction of the 5th metatarsal (in Jones fractures) often necessitates a longer immobilization period. *2-3 weeks* - This duration is generally too short for the adequate healing of most 5th metatarsal fractures, especially those that are **displaced** or involve the **watershed zone**. - A shorter period might be considered for very minor, stable **avulsion fractures** with minimal pain, but even then, a slightly longer protection might be advised. *16-20 weeks* - This length of time is typically reserved for **severe, complex fractures**, open fractures with complications, or cases requiring **multiple surgical interventions** and prolonged rehabilitation, which is not the standard for an uncomplicated 5th metatarsal fracture. - Such an extended period of immobilization could also lead to **significant muscle atrophy** and joint stiffness. *3-5 weeks* - While sometimes considered for **stable avulsion fractures** of the 5th metatarsal base or mild stress fractures, this period is often insufficient for complete healing of the more common and problematic **Jones fracture**. - Rushing the return to weight-bearing can increase the risk of **non-union** or refracture.
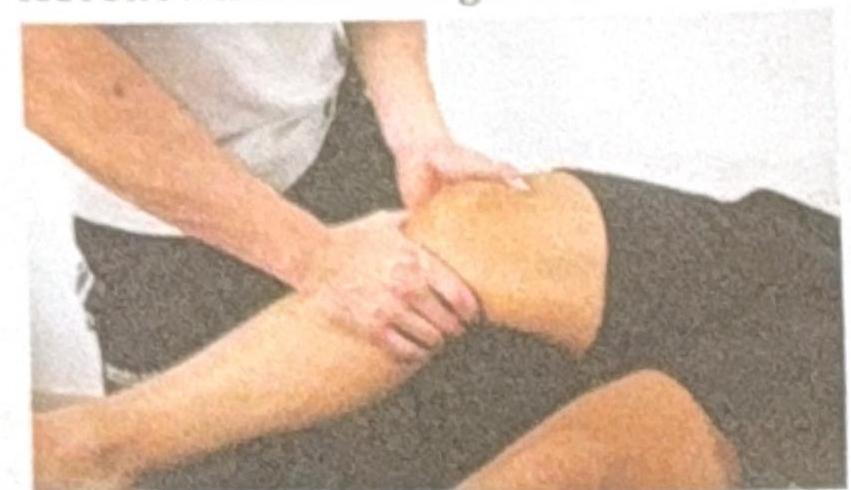
Question 5: A football player experienced a twist in the ankle and knee. Clinically, no bone injury was appreciated. The examiner is performing the test shown in the image. Which test is this?
- A. Posterior drawer for PCL
- B. McMurray
- C. Lachman (Correct Answer)
- D. Anterior drawer for ACL
Explanation: ***Lachman*** - The image shows the examiner holding the distal thigh and proximal tibia, with the knee flexed at a **20-30 degree angle**, applying an **anterior translational force** to the tibia. This specific maneuver is characteristic of the Lachman test. - The Lachman test is highly sensitive for detecting **anterior cruciate ligament (ACL) tears**, particularly in acute injuries, due to the reduced hamstring spasm compared to the anterior drawer test. *Posterior drawer for PCL* - The posterior drawer test involves flexing the knee to **90 degrees** and applying a **posterior force** to the tibia to assess the integrity of the **posterior cruciate ligament (PCL)**. - The position of the knee in the image (flexed at a shallower angle) and the direction of the applied force (anteriorly towards the femur) do not match the technique for a posterior drawer test. *McMurray* - The McMurray test is performed to evaluate **meniscal tears** by flexing, extending, and rotating the knee while applying a varus or valgus stress. - The maneuver in the image, involving direct anterior translation of the tibia with the knee in slight flexion, is not consistent with the McMurray test. *Anterior drawer for ACL* - While also testing the **ACL**, the anterior drawer test typically involves flexing the knee to **90 degrees** and sitting on the foot, then pulling the tibia anteriorly. - The knee flexion angle in the image is much shallower than 90 degrees, making it inconsistent with the standard anterior drawer test.
Question 6: The X-ray shows plating done for a fracture. How does this fracture heal?
- A. Primary healing (Correct Answer)
- B. Secondary healing
- C. Tertiary healing
- D. Distraction histiogenesis
Explanation: **Primary healing** - **Plating of a fracture** aims to achieve **absolute stability** at the fracture site, which facilitates primary bone healing. - In primary healing, there is **direct bone formation** across the fracture gap without the formation of a significant callus. *Secondary healing* - Secondary healing involves the formation of a **callus** (fibrous tissue, cartilage, and immature bone) to bridge the fracture gap. - This type of healing occurs in situations with **relative stability** and some micromotion at the fracture site, such as with casting or intramedullary nailing. *Tertiary healing* - **Tertiary healing** is not a recognized term in the context of fracture healing. - Bone healing typically involves either primary or secondary mechanisms depending on the stability achieved. *Distraction histiogenesis* - **Distraction histiogenesis** is the process by which new bone is formed between bone surfaces that are gradually pulled apart using an external fixator (**distraction osteogenesis**). - This is used in procedures like **limb lengthening** and is distinct from the direct healing of a fracture fixed with a plate.
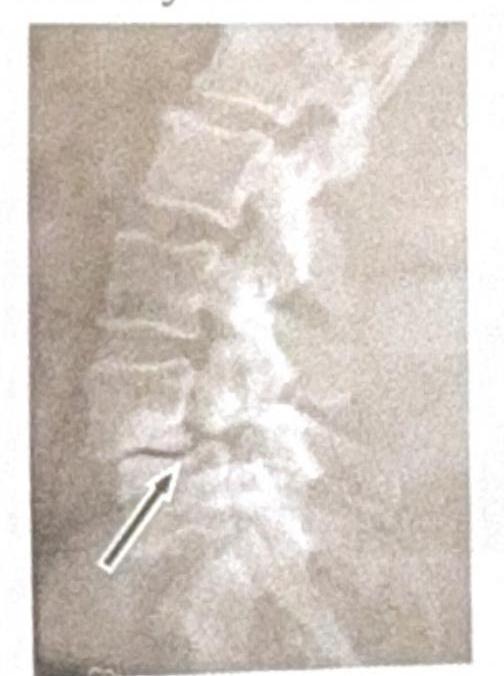
Question 7: Identify the condition shown in the image:
- A. Renal osteodystrophy
- B. Spondylolisthesis
- C. Tuberculosis (TB)
- D. Spondylolysis (Correct Answer)
Explanation: ***Spondylolysis*** * The image shows a **break in the pars interarticularis** of a vertebra, indicated by the arrow, which is characteristic of spondylolysis. * This condition is a **stress fracture** or defect in the pars interarticularis, a bony segment connecting the superior and inferior articular facets. *Renal osteodystrophy* * Renal osteodystrophy refers to a spectrum of **bone abnormalities** that occur in chronic kidney disease, not a specific vertebral fracture pattern. * It typically involves features such as **osteomalacia**, **osteitis fibrosa cystica**, or **osteoporosis**, which are not directly depicted as a fracture in this image. *Spondylolisthesis* * Spondylolisthesis is the **anterior slippage** of one vertebral body over another, which can be caused by bilateral spondylolysis but is not directly shown as a slip in this specific image. * The image distinctly highlights the **fracture line** itself, rather than the displacement of the vertebral body. *Tuberculosis (TB)* * Spinal tuberculosis (Pott's disease) typically presents with **destruction of vertebral bodies**, disc space narrowing, and often a **paravertebral abscess**. * The image does not show these features; instead, it demonstrates a clear **bony defect** in the pars interarticularis.
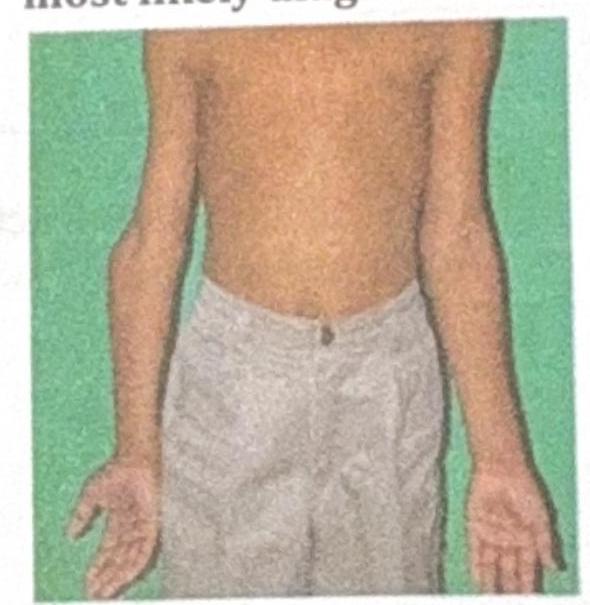
Question 8: A 10-year-old boy presents with the physical findings shown in the image, characterized by inward angulation of the elbows. What is the most likely diagnosis?
- A. Cubitus varus deformity (Correct Answer)
- B. Madelung deformity
- C. Nursemaid's elbow
- D. Klippel-Feil syndrome
Explanation: ***Cubitus varus deformity*** - The image clearly illustrates an **inward angulation of the elbow** (gunstock deformity), which is characteristic of **cubitus varus**. This often occurs after a supracondylar fracture of the humerus that heals with malunion. - This deformity typically results in a decreased or reversed carrying angle of the elbow. *Madelung deformity* - This is a rare congenital anomaly characterized by **dorsal and radial bowing of the distal radius** and premature fusion of the ulnar physis. - It primarily affects the wrist, leading to a visible prominence of the distal ulna and carpal bone subluxation, which is not depicted in the elbow region in the image. *Nursemaid's elbow* - This is a common injury in young children where the **radial head is subluxated** from the annular ligament, often due to a sudden pull on the forearm. - It presents as acute pain and refusal to use the arm, but does not involve a chronic structural deformity or angulation of the elbow joint as shown in the image. *Klippel-Feil syndrome* - This is a rare congenital disorder characterized by the **fusion of two or more cervical vertebrae**. - Its primary manifestations are a short neck, low posterior hairline, and restricted neck movement, with no direct involvement or deformity of the elbow joint itself.
Question 9: Fracture at which site affects the longitudinal growth of a bone?
- A. Epiphyseal plate (Correct Answer)
- B. Diaphysis
- C. Epiphysis
- D. Metaphysis
Explanation: ***Epiphyseal plate*** - The **epiphyseal plate**, also known as the **growth plate**, is a cartilaginous disc responsible for the **longitudinal growth** of long bones. - A fracture in this region can damage the **chondrocytes** and disrupt the normal ossification process, potentially leading to **growth arrest** or limb length discrepancies. *Diaphysis* - The **diaphysis** is the **shaft** or central part of a long bone. - While a fracture here can cause pain and instability, it typically does not directly affect the **longitudinal growth** potential of the bone. *Epiphysis* - The **epiphysis** is the end part of a long bone, initially separated from the main bone by cartilage but later fused with it. - Although it contains the epiphyseal plate in growing individuals, a fracture to the epiphysis itself (excluding the growth plate) primarily affects the **joint surface** and stability, rather than longitudinal growth directly. *Metaphysis* - The **metaphysis** is the transitional zone between the diaphysis and the epiphysis, adjacent to the growth plate. - While fractures in this area can be close to the growth plate, a metaphyseal fracture generally does not directly damage the **growth plate cartilage** to the same extent as a fracture through the plate itself, making its impact on longitudinal growth less direct or severe.
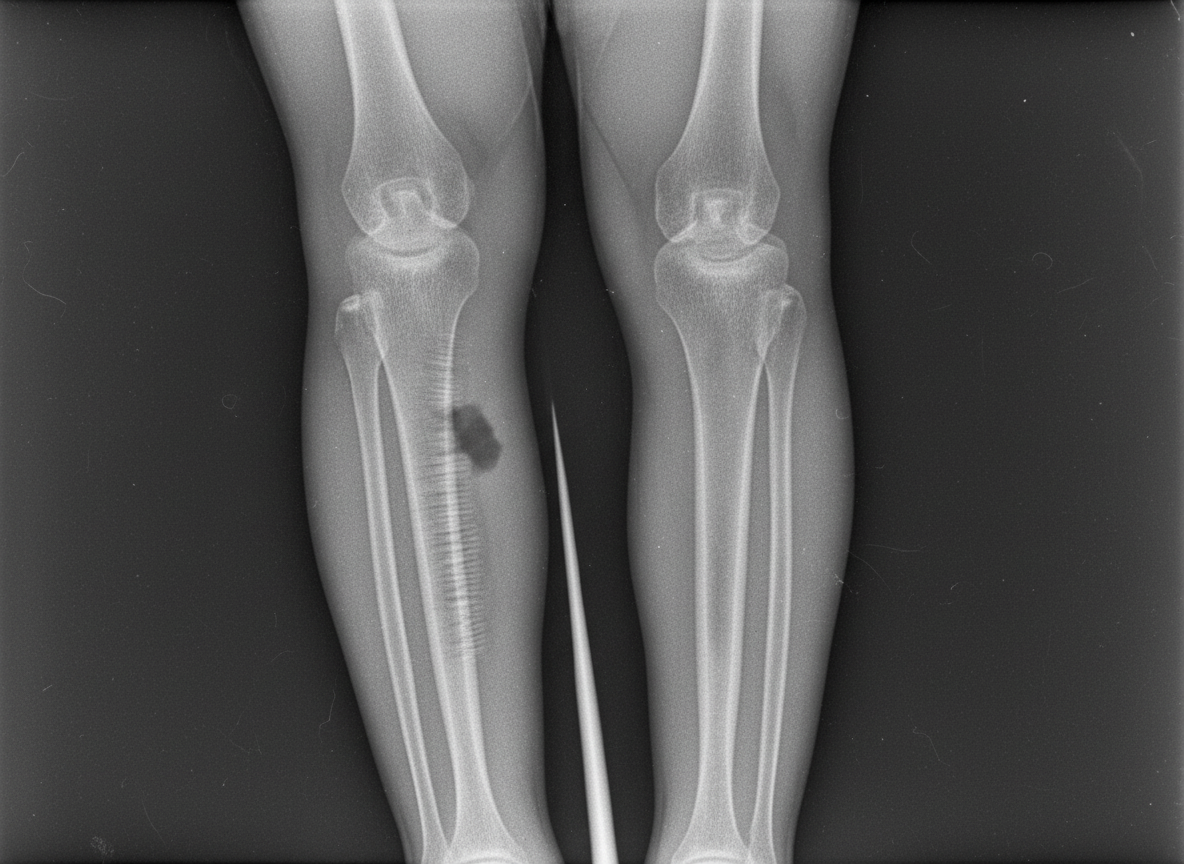
Question 10: An 18-year-old boy presents with tenderness, warmth over the bone, and fever, ESR and CRP levels. The radiograph is shown below. What is the most likely diagnosis?
- A. Ewing's sarcoma
- B. Osteosarcoma
- C. Osteomyelitis (Correct Answer)
- D. Giant cell tumor
Explanation: ***Osteomyelitis*** - The presentation of **tenderness**, **warmth over the bone**, **fever**, and elevated **ESR** and **CRP** are classic signs of a bone infection, or osteomyelitis. - While not explicitly shown in the provided text, a radiograph in acute osteomyelitis might show **soft tissue swelling** or subtle **periosteal elevation**, progressing to **bone destruction** and **sclerosis** in later stages. *Ewing's sarcoma* - This is a highly malignant bone tumor that presents with **pain** and **swelling**, but is typically not associated with a pronounced **fever** and signs of systemic infection. - Radiographically, it often shows an "onion-skin" **periosteal reaction** and lytic lesions, without the strong inflammatory markers seen here. *Osteosarcoma* - This is another malignant bone tumor, primarily presenting with bone **pain** and **swelling**, but systemic inflammatory signs like **fever** are rare unless there is a pathologic fracture or infection secondary to tumor necrosis. - Radiographs typically show a "sunburst" appearance, **Codman's triangle**, or mixed lytic and blastic lesions, not indicative of acute infection. *Giant cell tumor* - This is a usually **benign aggressive bone tumor** that causes **pain** and **swelling** around joints. - It does not typically present with systemic signs of infection such as **fever** and significantly elevated **ESR** and **CRP** unless there is a secondary infection, and it usually affects the **epiphyses** of long bones in young adults.