A person with a history of chronic alcohol consumption who indulged in binge drinking 10 days ago is brought to the emergency department in an unconscious state. A non-contrast CT scan was normal, and his blood glucose level is 45 mg/dL. What is the most appropriate treatment?
Q22
A 35-year-old male from a rural village in South Asia is admitted to the hospital with a 5-day history of high-grade fever, severe headache, and progressive breathlessness. His family reports that he has become increasingly disoriented over the past 48 hours, with episodes of confusion and drowsiness. Upon examination, the patient is febrile with a temperature of 39°C (102.2°F), tachypneic with a respiratory rate of 30 breaths per minute, and is displaying signs of altered mental status, including lethargy and difficulty following commands. His oxygen saturation is 92% on room air. There are no signs of a rash or bleeding. What is the diagnosis?
Q23
A patient presents with features of heart failure. On examination, an irregularly irregular pulse is noted, and the patient has a loud diastolic sound. The jugular venous pressure (JVP) shows a rapid Y descent. What is the most likely diagnosis?
Q24
274. A young athlete was found to have hypertrophic cardiomyopathy during testing for a competitive sport. Which of the following maneuvers will increase the murmur?
Q25
Match the following
A. Atrial fibrillation
B. Atrial flutter
C. PSVT
D. Ventricular tachycardia
NEET-PG 2024 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 21: A person with a history of chronic alcohol consumption who indulged in binge drinking 10 days ago is brought to the emergency department in an unconscious state. A non-contrast CT scan was normal, and his blood glucose level is 45 mg/dL. What is the most appropriate treatment?
A. Normal saline
B. IM thiamine followed by dextrose (Correct Answer)
C. 5% dextrose/vitamin K
D. 25% dextrose
E. IV dextrose followed by thiamine
Explanation: **IM thiamine followed by dextrose**
- Administering **thiamine** prior to **dextrose** is crucial in patients with chronic alcohol use to prevent **Wernicke-Korsakoff syndrome**, as glucose administration can precipitate or worsen Wernicke encephalopathy in thiamine-deficient individuals.
- The patient's **hypoglycemia** (45 mg/dL) requires immediate correction with **dextrose**, but **thiamine** must be given first due to the patient's history of chronic alcohol consumption.
*Normal saline*
- While **normal saline** is used for rehydration and volume expansion, it does not address the patient's immediate and life-threatening **hypoglycemia** or **thiamine deficiency**.
- Without addressing **hypoglycemia**, the patient's unconscious state will persist and lead to further neurological damage.
*5% dextrose/vitamin K*
- **5% dextrose** alone might correct **hypoglycemia**, but administering it without prior **thiamine** in a chronic alcoholic can precipitate **Wernicke encephalopathy**.
- **Vitamin K** is typically given for coagulopathies or bleeding disorders, not as a primary treatment for **hypoglycemia** or **alcohol-related neurological emergencies** unless specific indications are present.
*25% dextrose*
- **25% dextrose** would rapidly correct **hypoglycemia**, but as with 5% dextrose, administering it without prior **thiamine** in a chronic alcoholic can precipitate or worsen **Wernicke encephalopathy**.
- The primary concern in this context for an alcoholic patient with hypoglycemia is the potential for **thiamine deficiency**.
*IV dextrose followed by thiamine*
- While this option includes both necessary treatments, the **incorrect sequence** is critical—administering **dextrose before thiamine** in a chronic alcoholic can precipitate **Wernicke encephalopathy**.
- The correct protocol requires **thiamine first** to replenish stores before glucose metabolism is accelerated by dextrose administration.
Question 22: A 35-year-old male from a rural village in South Asia is admitted to the hospital with a 5-day history of high-grade fever, severe headache, and progressive breathlessness. His family reports that he has become increasingly disoriented over the past 48 hours, with episodes of confusion and drowsiness. Upon examination, the patient is febrile with a temperature of 39°C (102.2°F), tachypneic with a respiratory rate of 30 breaths per minute, and is displaying signs of altered mental status, including lethargy and difficulty following commands. His oxygen saturation is 92% on room air. There are no signs of a rash or bleeding. What is the diagnosis?
A. Ebola
B. Zika
C. Malaria
D. NIPAH (Correct Answer)
E. Japanese Encephalitis
Explanation: ***NIPAH***
- The combination of **rapidly progressive encephalitis** (disorientation, confusion, lethargy), **respiratory distress** (breathlessness, tachypnea, reduced O2 saturation), and **geographical context** (rural South Asia) strongly points towards NIPAH virus infection.
- **Bats** (specifically fruit bats) are the natural reservoir for NIPAH virus, and exposure to bat secretions or contaminated food can lead to outbreaks, especially in rural areas where the image suggests bats are present.
- The **distinctive combination of severe respiratory and neurological symptoms** with rapid progression is characteristic of NIPAH.
*Ebola*
- Ebola typically presents with **hemorrhagic fever**, characterized by severe bleeding (both internal and external), which is not described in the patient's symptoms.
- While it causes high fever and altered mental status, the **prominent respiratory symptoms and lack of bleeding** make Ebola less likely.
*Zika*
- Zika virus infection is usually **mild or asymptomatic** and primarily transmitted by mosquitoes.
- While encephalitis can occur in rare cases, the **severe respiratory distress and rapid progression of neurological symptoms** described are not typical for Zika.
*Malaria*
- Malaria is characterized by **cyclic fevers, chills, and sweats**, and can cause severe symptoms like cerebral malaria leading to altered mental status.
- However, the patient's **pronounced respiratory symptoms and rapid onset of encephalitis without typical cyclic fever patterns** make malaria a less fitting diagnosis than NIPAH.
*Japanese Encephalitis*
- Japanese Encephalitis is endemic in South Asia and does cause **encephalitis with altered mental status**.
- However, **prominent respiratory distress and breathlessness** are not typical features of Japanese Encephalitis, which primarily affects the central nervous system.
- The **rapid progression with severe respiratory involvement** points more toward NIPAH than Japanese Encephalitis.
Question 23: A patient presents with features of heart failure. On examination, an irregularly irregular pulse is noted, and the patient has a loud diastolic sound. The jugular venous pressure (JVP) shows a rapid Y descent. What is the most likely diagnosis?
A. Constrictive pericarditis
B. Cardiac tamponade
C. Mitral stenosis (Correct Answer)
D. Aortic regurgitation
E. Mitral regurgitation
Explanation: ***Mitral stenosis***
- An **irregularly irregular pulse** suggests **atrial fibrillation**, a common complication of mitral stenosis due to left atrial enlargement.
- A **loud diastolic sound**, also known as an **opening snap**, is characteristic of a stenotic mitral valve as it opens, occurring early in diastole.
- The **rapid Y descent** on JVP can occur due to elevated right-sided pressures from pulmonary hypertension secondary to mitral stenosis.
*Constrictive pericarditis*
- While it can cause heart failure and an elevated JVP with a rapid Y descent (**Friedreich's sign**), the description of an "irregularly irregular pulse" and a "loud diastolic sound" (opening snap) is not typical.
- The loud diastolic sound in constrictive pericarditis would be a **pericardial knock**, which is usually later than an opening snap and less distinct.
*Cardiac tamponade*
- Characterized by **Beck's triad** (hypotension, muffled heart sounds, elevated JVP) and often presents with **pulsus paradoxus**.
- The JVP in tamponade typically shows an **absent or diminished Y descent**, due to impaired ventricular filling from external compression.
*Aortic regurgitation*
- Causes a **diastolic murmur**, but not a loud diastolic sound or opening snap.
- The pulse is often a **collapsing pulse** or **water-hammer pulse**, and it is not typically irregularly irregular unless atrial fibrillation or another arrhythmia is co-existent.
*Mitral regurgitation*
- Can cause heart failure and atrial fibrillation, but the characteristic finding is a **pansystolic murmur**, not a loud diastolic sound.
- There is no opening snap in mitral regurgitation; instead, there may be an **S3 gallop** in severe cases.
- The rapid Y descent is less prominent compared to mitral stenosis.
Question 24: 274. A young athlete was found to have hypertrophic cardiomyopathy during testing for a competitive sport. Which of the following maneuvers will increase the murmur?
A. Handgrip
B. Valsalva maneuver (Correct Answer)
C. Squatting
D. Leaning forward
E. Passive leg raise
Explanation: **Valsalva maneuver**
- The **Valsalva maneuver** reduces **preload** by decreasing venous return to the heart.
- A decrease in preload reduces the left ventricular chamber size, which in turn exacerbates the **left ventricular outflow tract (LVOT) obstruction** characteristic of hypertrophic cardiomyopathy (HCM), thereby **increasing the intensity of the murmur**.
*Handgrip*
- **Handgrip** is an isometric exercise that leads to an increase in **afterload** and **peripheral vascular resistance**.
- Increased afterload causes the left ventricle to eject blood against higher pressure, which **enlarges the left ventricular chamber** and **reduces the LVOT obstruction**, thus **decreasing the intensity of the murmur** in HCM.
*Squatting*
- **Squatting** increases both **preload** (due to increased venous return) and **afterload** (due to increased peripheral vascular resistance).
- The increased preload and afterload lead to an **increased left ventricular volume**, which **reduces the LVOT obstruction** and therefore **decreases the intensity of the murmur** in HCM.
*Passive leg raise*
- **Passive leg raise** increases **preload** by increasing venous return to the heart from the lower extremities.
- The increased preload leads to an **increased left ventricular chamber size**, which **reduces the LVOT obstruction** and therefore **decreases the intensity of the murmur** in HCM.
*Leaning forward*
- Leaning forward during auscultation is typically used to better hear **aortic regurgitation murmurs**, as it brings the aorta closer to the chest wall.
- This maneuver does not significantly alter **cardiac preload or afterload** in a way that would consistently increase the murmur of hypertrophic cardiomyopathy.
Question 25: Match the following
A. Atrial fibrillation
B. Atrial flutter
C. PSVT
D. Ventricular tachycardia
A. A-1, B-2, C-3, D-4
B. A-2, B-1, C-3, D-4 (Correct Answer)
C. A-1, B-2, C-4, D-3
D. A-4, B-3, C-2, D-1
E. A-2, B-1, C-4, D-3
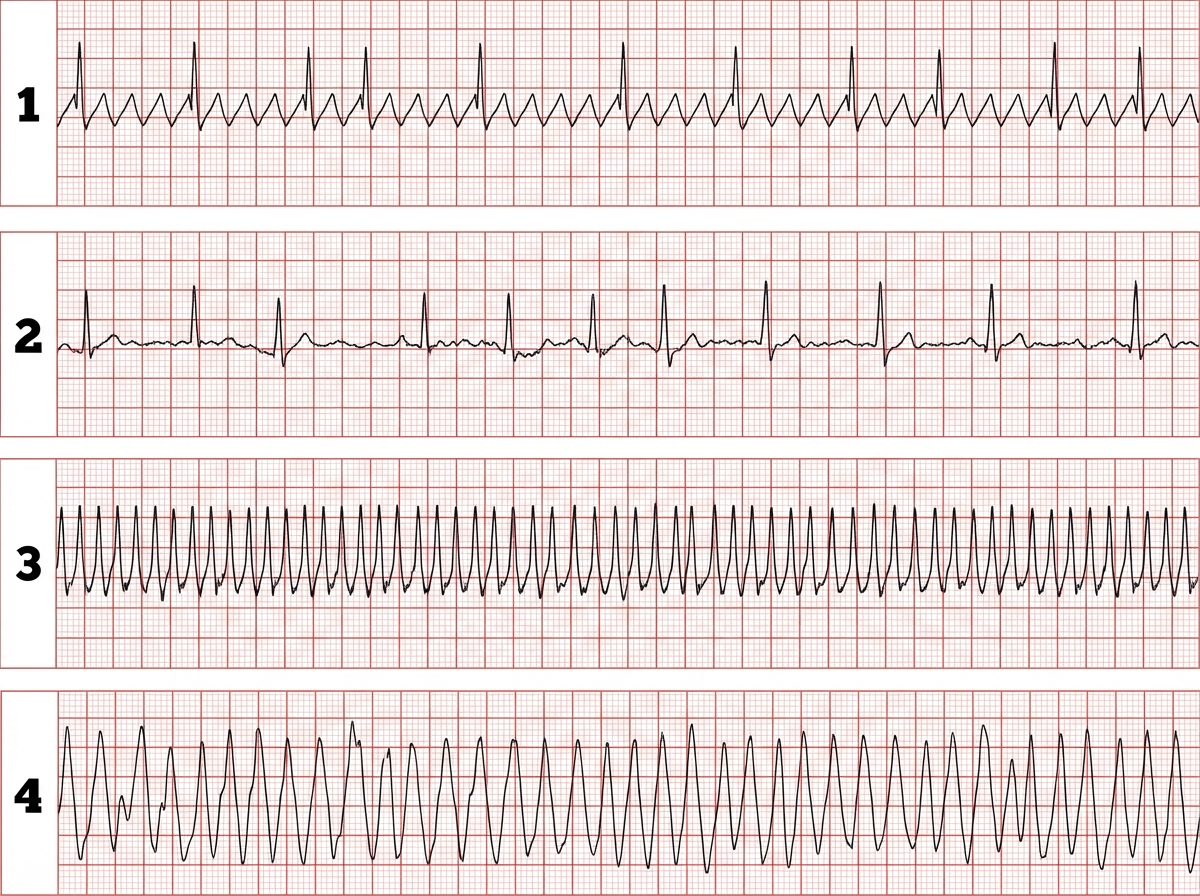
Explanation: ***A-2, B-1, C-3, D-4***
- Image 2 shows irregularly irregular QRS complexes with no discernible P waves, which is characteristic of **atrial fibrillation**.
- Image 1 shows a "sawtooth" pattern of atrial activity, indicative of **atrial flutter**.
- Image 3 displays a narrow complex tachycardia with a very regular rhythm, consistent with **PSVT**.
- Image 4 demonstrates wide, regular QRS complexes without clear P waves, which is the hallmark of **ventricular tachycardia**.
*A-1, B-2, C-3, D-4*
- This option incorrectly matches atrial fibrillation with the "sawtooth" pattern (image 1) and atrial flutter with the irregularly irregular rhythm (image 2).
- Atrial fibrillation is characterized by the absence of discrete P waves and irregular ventricular response (image 2), while atrial flutter shows organized atrial activity with a "sawtooth" pattern (image 1).
*A-1, B-2, C-4, D-3*
- This option misidentifies image 1 as atrial fibrillation and image 2 as atrial flutter, which are reversed.
- It also incorrectly matches PSVT with image 4 (ventricular tachycardia) and ventricular tachycardia with image 3 (PSVT).
*A-2, B-1, C-4, D-3*
- This option correctly identifies atrial fibrillation (A-2) and atrial flutter (B-1), but incorrectly swaps the ventricular and supraventricular tachycardias.
- Image 3 shows narrow complex tachycardia (PSVT), not the wide complex pattern of ventricular tachycardia seen in image 4.
*A-4, B-3, C-2, D-1*
- This option incorrectly matches all the rhythms to the wrong images, demonstrating a fundamental misunderstanding of their characteristic ECG features.
- For example, it matches atrial fibrillation to image 4 (ventricular tachycardia) and ventricular tachycardia to image 1 (atrial flutter).