All SubjectsAnatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q11
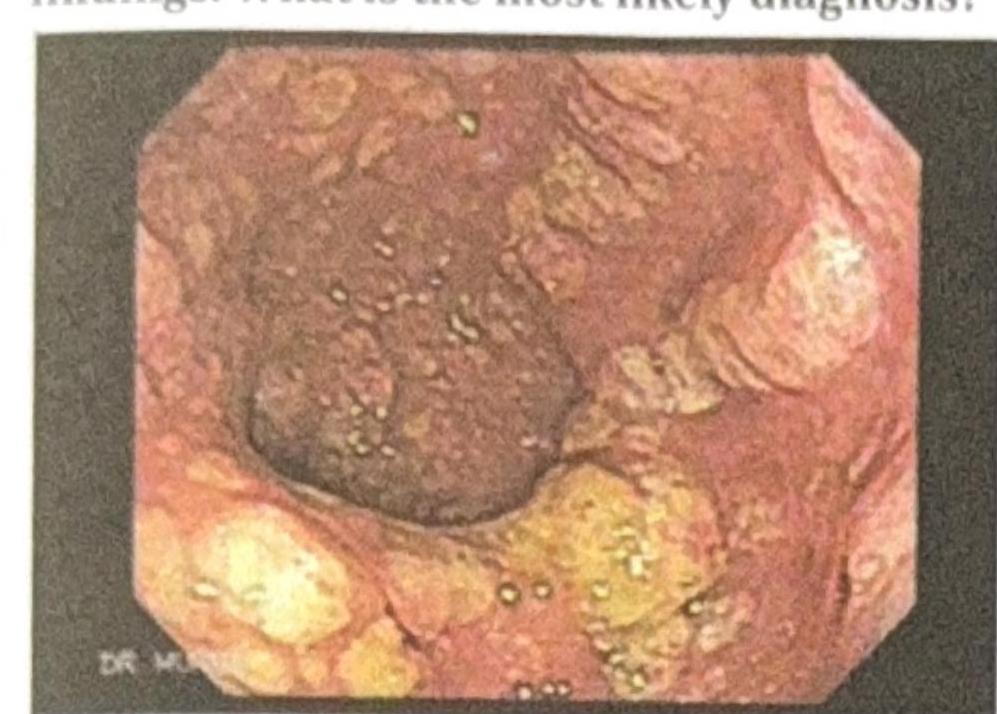
A patient presents to the OPD with recurrent diarrhea, abdominal pain, and foul-smelling stools. The colonoscopy reveals the following findings. What is the most likely diagnosis?
Q12
An alcoholic patient presents with a wide-based gait and nystagmus after a road traffic accident (RTA). Which lobe of the cerebellum is most likely affected?
Q13
A patient living with HIV presents with foulsmelling stools. Microscopic examination of the stool reveals no cysts or ova, but a 200-micrometer larva is observed. What is the most likely pathogen?
Q14
Which of the following statements is correct about Paroxysmal Nocturnal Hemoglobinuria (PNH)?
Q15
A patient presents with pulmonary hemorrhage and is P-ANCA positive. What is the most likely diagnosis?
Q16
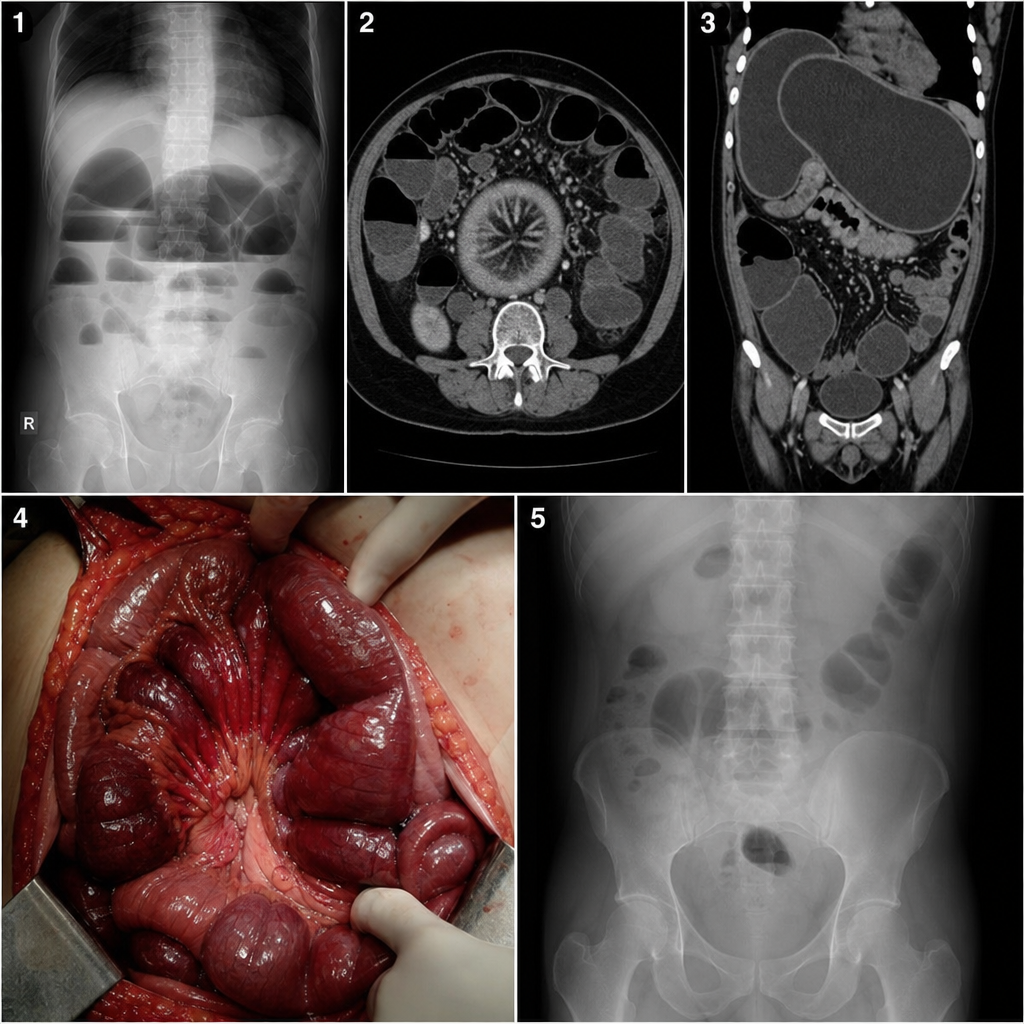
Which of the following options shows the correct order?
Q17
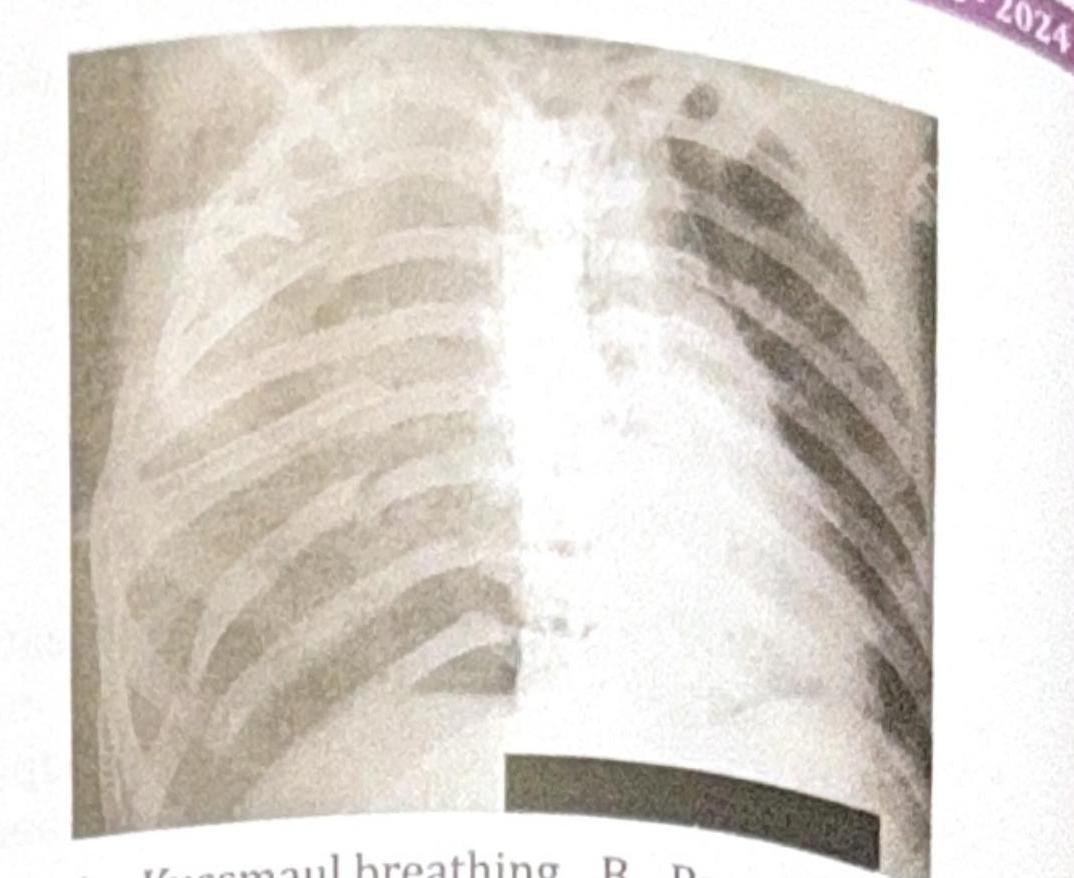
A 25-year-old patient presents with acute epigastric pain and elevated serum lipase. The patient was stabilized after 3 days, and a chest X-ray was obtained. What is the most common pulmonary complication associated with this condition?
Q18
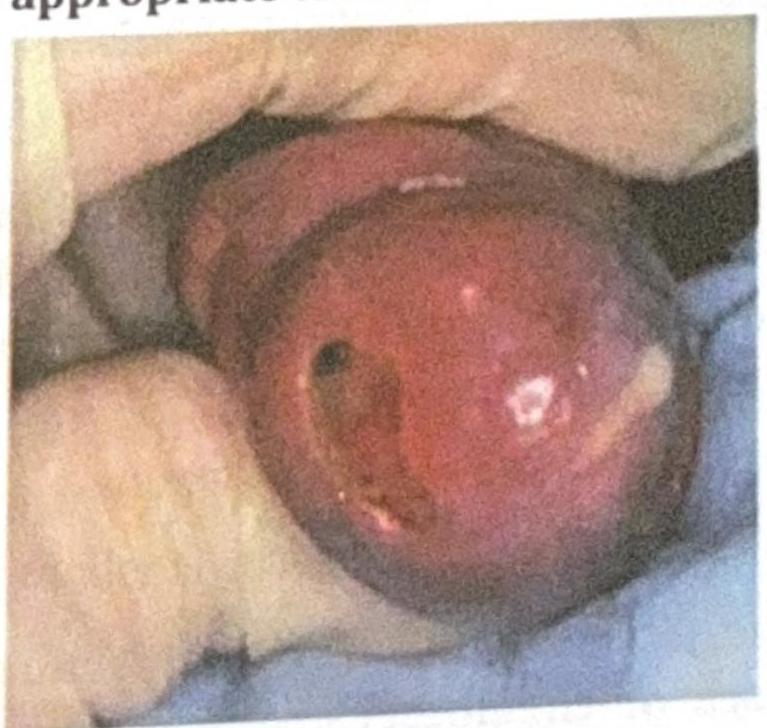
An adult man presents with the clinical condition shown in the image, and a Gram stain reveals Gram-negative diplococci. What is the most appropriate treatment?
Q19
A 45-year-old male presents to the emergency department following a motor vehicle accident. He complains of severe chest pain and difficulty breathing. On examination, he appears distressed, with a respiratory rate of 28 breaths per minute. His oxygen saturation is 88% on room air. There is visible bruising on the chest, X-ray is done which is shown below. Which of the following is seen in this patient?