NEET-PG 2024 — Internal Medicine
25 Previous Year Questions with Answers & Explanations
Match the following ECG findings (1-4) with their corresponding arrhythmias (A-D): 1. Sawtooth pattern in leads II, III, aVF with regular ventricular response 2. Irregularly irregular rhythm with absent P waves 3. Narrow QRS tachycardia with abrupt onset/termination 4. Wide QRS tachycardia with AV dissociation A. Atrial fibrillation B. PSVT (Paroxysmal Supraventricular Tachycardia) C. Atrial flutter D. Ventricular tachycardia What is the correct matching?
A patient is pulseless with the following rhythm shown in the ECG. What is the next best step in management?
A hypertensive patient presents with an irregularly irregular pulse and a loud P2 on auscultation. Which JVP finding is likely to be seen in this patient?
A 60-year-old lady presents with shortness of breath (SOB) and episodes of angina pectoris. Work-up reveals aortic stenosis. Which of the following is the most likely reason behind these chest pain episodes?
A patient presents with wheezing that improves with as-needed use of albuterol. Spirometry shows FEV1 ranging from 70 % to 83 %, and the patient experiences nighttime chest tightening twice a week. What is the most appropriate treatment?
A patient presents with hypotension, hyponatremia, and blackening of the palmar creases. Which of the following conditions is most likely associated with these symptoms?
A young patient in an endemic area presents with pleural fluid showing LDH level greater than 0.6 times the serum LDH, protein level greater than 0.5 times the serum protein, and lymphocytic predominance. What is the most likely diagnosis?
A patient presents with acute epigastric pain and an increase in serum lipase. Several days after stabilization, a chest X-ray shows bilateral diffuse infiltrates. What is the most common pathology explaining the chest X-ray findings?

A patient with a history of hypertension presents with atrial fibrillation, shortness of breath, and bilateral basal crackles on auscultation. Which of the following would be the least important in the management of this patient?
In Type 1 Diabetes Mellitus (DM) stage 3 beta cell destruction, which of the following is the most likely presentation?
NEET-PG 2024 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 1: Match the following ECG findings (1-4) with their corresponding arrhythmias (A-D): 1. Sawtooth pattern in leads II, III, aVF with regular ventricular response 2. Irregularly irregular rhythm with absent P waves 3. Narrow QRS tachycardia with abrupt onset/termination 4. Wide QRS tachycardia with AV dissociation A. Atrial fibrillation B. PSVT (Paroxysmal Supraventricular Tachycardia) C. Atrial flutter D. Ventricular tachycardia What is the correct matching?
- A. A-2, B-1, C-3, D-4
- B. A-1, B-2, C-4, D-3
- C. A-2, B-3, C-1, D-4 (Correct Answer)
- D. A-4, B-3, C-2, D-1
- E. A-1, B-2, C-3, D-4
Explanation: The correct matching is **A-2, B-3, C-1, D-4**: ***C-1: Atrial flutter - Sawtooth pattern*** - Atrial flutter is characterized by a **sawtooth pattern** of flutter waves, particularly prominent in leads II, III, and aVF - Represents rapid, organized atrial depolarization at 250-350 bpm - Regular ventricular response due to **AV block** (commonly 2:1 or 4:1) - The sawtooth pattern is the pathognomonic feature ***A-2: Atrial fibrillation - Irregularly irregular rhythm*** - Identified by an **irregularly irregular rhythm** with absent distinct P waves - Replaced by chaotic fibrillatory waves showing disorganized atrial activity - Ventricular rate is rapid and unpredictable - No organized atrial pattern unlike the regular flutter waves ***B-3: PSVT - Narrow QRS with abrupt onset/termination*** - Presents with **narrow QRS complex tachycardia** (QRS < 0.12 seconds) with regular rhythm - Atrial rate usually 150-250 bpm - **Abrupt onset and termination** is the characteristic feature differentiating it from other supraventricular arrhythmias - P waves may be hidden within or immediately after QRS complexes ***D-4: Ventricular tachycardia - Wide QRS with AV dissociation*** - Defined by **wide QRS complex tachycardia** (QRS > 0.12 seconds) - **AV dissociation** is a key diagnostic feature showing independent atrial and ventricular activity - Originates from ventricular tissue, not supraventricular structures - Lacks the organized P wave patterns seen in atrial arrhythmias
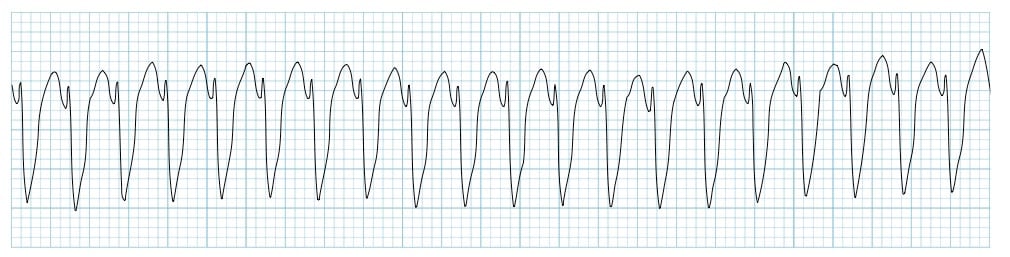
Question 2: A patient is pulseless with the following rhythm shown in the ECG. What is the next best step in management?
- A. Defibrillate and continue chest compression (Correct Answer)
- B. Defibrillate and check pulse
- C. Check pulse and give synchronized DC
- D. Give synchronized DC and continue chest compressions
- E. Start chest compressions and give epinephrine
Explanation: ***Defibrillate and continue chest compression*** - This scenario describes a **pulseless ventricular tachycardia (pVT)**, which is a **shockable rhythm**. - Immediate defibrillation is crucial, followed by resuming **chest compressions** without delay, as per advanced cardiac life support (ACLS) guidelines. - The correct sequence is: shock → immediate CPR for 2 minutes → rhythm/pulse check. *Defibrillate and check pulse* - While defibrillation is the correct initial intervention for a shockable rhythm, checking the pulse immediately after is incorrect. - Chest compressions should be resumed immediately after a shock for 2 minutes before stopping to check a pulse. - Minimizing interruptions in chest compressions is critical for survival. *Check pulse and give synchronized DC* - Checking a pulse before any intervention wastes critical time in a pulseless patient with a shockable rhythm; immediate defibrillation is indicated. - Synchronized direct current (DC) cardioversion is used for unstable patients **with a pulse** (e.g., unstable ventricular tachycardia with a pulse), not for pulseless rhythms. *Give synchronized DC and continue chest compressions* - Synchronized DC cardioversion is inappropriate for a **pulseless rhythm**; unsynchronized defibrillation is required. - Synchronization requires an R wave to time the shock, which is not feasible in pulseless VT management. *Start chest compressions and give epinephrine* - While chest compressions are essential, the **immediate priority** for a shockable rhythm (pVT/VF) is **defibrillation**. - Epinephrine is given during CPR cycles (after the first shock), but defibrillation must come first for shockable rhythms. - This would be the approach for **non-shockable rhythms** (PEA/asystole), not pulseless VT.
Question 3: A hypertensive patient presents with an irregularly irregular pulse and a loud P2 on auscultation. Which JVP finding is likely to be seen in this patient?
- A. Absent a wave (Correct Answer)
- B. Cannon a wave
- C. Rapid $x$ descent
- D. Rapid $y$ descent
- E. Prominent v wave
Explanation: ***Absent a wave*** - An **irregularly irregular pulse** and **loud P2** suggest **atrial fibrillation** with **pulmonary hypertension**. In atrial fibrillation, there is chaotic atrial activity, meaning the atria do not contract in a coordinated fashion. - The **"a" wave** on the JVP tracing represents **atrial contraction**. Since the atria are fibrillating and not contracting effectively, the normal "a" wave will be absent. *Cannon a wave* - **Cannon a waves** occur when the **right atrium contracts against a closed tricuspid valve**, such as during **ventricular tachycardia** or **complete heart block** (AV dissociation). - This patient's irregularly irregular pulse suggests **atrial fibrillation**, not a condition typically associated with cannon a waves. *Rapid $x$ descent* - A **rapid x descent** primarily reflects **atrial relaxation** and **right ventricular systole**, which pulls the tricuspid annulus downwards. - While a rapid x descent can be seen in various conditions, it is not the most specific JVP finding for the described clinical picture, which points strongly to absent atrial contraction. *Rapid $y$ descent* - A **rapid y descent** signifies rapid filling of the right ventricle during early diastole, often associated with a **compliant right ventricle** and unobstructed tricuspid inflow. It can be prominent in conditions like **constrictive pericarditis** or **restrictive cardiomyopathy**. - This finding is not directly or specifically linked to the irregularly irregular pulse and absent atrial contraction seen in atrial fibrillation. *Prominent v wave* - A **prominent v wave** occurs with **tricuspid regurgitation**, where blood regurgitates back into the right atrium during ventricular systole, causing venous distension. - While pulmonary hypertension can eventually lead to right ventricular dysfunction and tricuspid regurgitation, the most characteristic JVP finding for **atrial fibrillation itself** is the **absence of the "a" wave** due to lack of coordinated atrial contraction.
Question 4: A 60-year-old lady presents with shortness of breath (SOB) and episodes of angina pectoris. Work-up reveals aortic stenosis. Which of the following is the most likely reason behind these chest pain episodes?
- A. Increased pressure in aorta
- B. Decreased pressure in aorta
- C. Increased oxygen consumption in the heart (Correct Answer)
- D. Increase in volume overload of the heart
- E. Decreased coronary blood flow
Explanation: ***Increased oxygen consumption in the heart*** - In **aortic stenosis**, the left ventricle must generate significantly higher pressures to eject blood through the narrowed aortic valve, leading to **left ventricular hypertrophy**. This increased workload significantly raises the **myocardial oxygen demand**. - Angina pectoris occurs when this increased oxygen demand surpasses the oxygen supply, leading to **myocardial ischemia**. - This is the **primary mechanism** of angina in aortic stenosis. *Increased pressure in aorta* - While there is **increased pressure within the left ventricle** to overcome the stenotic valve, the pressure in the aorta *distal* to the stenosis is often normal or even slightly reduced due to the obstruction. - Increased aortic pressure itself is not the primary direct cause of angina in aortic stenosis; rather, it's the compensatory ventricular workload. *Decreased pressure in aorta* - A **decreased pressure in the aorta** could actually worsen coronary perfusion, but the primary reason for angina in aortic stenosis is the vastly **increased myocardial demand**, not necessarily a critical drop in aortic pressure. - The elevated left ventricular pressure required to overcome the stenosis is the key factor driving the angina. *Increase in volume overload of the heart* - **Aortic stenosis primarily causes pressure overload**, not volume overload, on the left ventricle due to the obstruction to outflow. - Volume overload typically occurs in conditions like **aortic regurgitation** or **mitral regurgitation**, which have different pathophysiological mechanisms for angina. *Decreased coronary blood flow* - While **decreased coronary perfusion** can be a contributing factor in aortic stenosis (due to reduced aortic pressure and shortened diastolic filling time), it is a **secondary mechanism**. - The **primary cause** of angina in aortic stenosis is the markedly **increased myocardial oxygen demand** from left ventricular hypertrophy and increased workload, rather than a primary reduction in coronary blood flow.
Question 5: A patient presents with wheezing that improves with as-needed use of albuterol. Spirometry shows FEV1 ranging from 70 % to 83 %, and the patient experiences nighttime chest tightening twice a week. What is the most appropriate treatment?
- A. Continue with albuterol
- B. Replace with salmeterol twice daily
- C. Start Tab prednisolone
- D. Add an inhaled corticosteroid (Correct Answer)
- E. Add a leukotriene modifier
Explanation: ***Add an inhaled corticosteroid*** * The patient has persistent asthma as evidenced by symptoms occurring twice a week (nighttime chest tightening), and **FEV1 variability** despite current albuterol use. * Adding a **low-dose inhaled corticosteroid** is the recommended *first-line controller treatment* for persistent asthma to reduce inflammation and prevent exacerbations per **GINA guidelines**. *Continue with albuterol* * Continuing albuterol alone is insufficient for persistent asthma, as it only provides **symptomatic relief** and does not address the underlying inflammation. * This approach would lead to continued symptoms and potential **asthma exacerbations**. *Replace with salmeterol twice daily* * Salmeterol is a **long-acting beta-agonist (LABA)**, and while it provides prolonged bronchodilation, it should never be used as monotherapy in asthma due to the risk of severe exacerbations. * LABAs should always be prescribed in combination with an **inhaled corticosteroid**. *Start Tab prednisolone* * **Oral prednisolone** is a systemic corticosteroid typically reserved for **severe asthma exacerbations** or for patients whose symptoms are not controlled by high-dose inhaled corticosteroids and other controller medications. * It carries more significant **side effects** with long-term use compared to inhaled corticosteroids. *Add a leukotriene modifier* * While **leukotriene receptor antagonists** (e.g., montelukast) can be used as alternative controller therapy for mild persistent asthma, they are considered **less effective** than inhaled corticosteroids. * They are typically reserved as an alternative for patients who cannot use or tolerate inhaled corticosteroids, or as **add-on therapy** in more severe cases.
Question 6: A patient presents with hypotension, hyponatremia, and blackening of the palmar creases. Which of the following conditions is most likely associated with these symptoms?
- A. Conn syndrome
- B. Cushing's syndrome
- C. Primary ACTH deficiency
- D. Addison disease (Correct Answer)
- E. Sheehan syndrome
Explanation: ***Addison disease*** - **Hypotension**, **hyponatremia**, and **hyperpigmentation** (blackening of palmar creases) are classic symptoms of **primary adrenal insufficiency** or Addison disease, due to deficient cortisol and aldosterone. - The lack of **cortisol** leads to hypotension and fatigue, while the absence of **aldosterone** causes hyponatremia and hyperkalemia. *Conn syndrome* - This condition involves **primary hyperaldosteronism**, typically leading to **hypertension** and **hypokalemia**, which contradicts the patient's symptoms of hypotension and hyponatremia. - Pigmentation changes are not a feature of Conn syndrome. *Cushing's syndrome* - Characterized by **excess cortisol**, leading to symptoms like **hypertension**, **hyperglycemia**, and central obesity, not hypotension or hyperpigmentation. - **Hyponatremia** is also not typical in Cushing's syndrome. *Primary ACTH deficiency* - Also known as **secondary adrenal insufficiency**, this condition results in low cortisol but typically spares aldosterone production, meaning **hyponatremia** and **hyperkalemia** are less common. - **Hyperpigmentation** does not occur in primary ACTH deficiency because ACTH levels are low. *Sheehan syndrome* - This is **postpartum pituitary necrosis** causing panhypopituitarism, which can lead to secondary adrenal insufficiency with hypotension and hyponatremia. - However, **hyperpigmentation does not occur** in Sheehan syndrome because ACTH levels are low (secondary insufficiency), not elevated as in Addison disease. - The clinical context would typically include a history of postpartum hemorrhage and failure to lactate.
Question 7: A young patient in an endemic area presents with pleural fluid showing LDH level greater than 0.6 times the serum LDH, protein level greater than 0.5 times the serum protein, and lymphocytic predominance. What is the most likely diagnosis?
- A. Tuberculosis (Correct Answer)
- B. Heart failure
- C. Hepatic failure
- D. Renal failure
- E. Malignancy
Explanation: ***Tuberculosis*** - The patient's presentation with **exudative pleural fluid** (LDH > 0.6 times serum LDH, protein > 0.5 times serum protein) in an **endemic area** strongly suggests tuberculosis. - The **lymphocytic predominance** in the pleural fluid is a hallmark characteristic of tuberculous pleurisy. - **Young age** and **endemic area** further support TB as the most likely diagnosis. *Heart failure* - Pleural effusions due to heart failure are typically **transudative**, meaning they have low protein and LDH levels. - While heart failure can lead to pleural effusions, the fluid characteristics (exudative, lymphocytic predominance) do not fit this diagnosis. *Hepatic failure* - Pleural effusions in hepatic failure (e.g., due to cirrhosis) are usually **transudative** and result from fluid shifting from the abdomen (hepatic hydrothorax). - The fluid analysis in this scenario (exudative, lymphocytic predominance) is inconsistent with hepatic failure. *Renal failure* - Pleural effusions associated with renal failure (e.g., uremic pleurisy) can be exudative, but they often present with a **neutrophilic predominance** or may be hemorrhagic. - The specific lymphocytic predominance points away from typical renal failure-associated effusions. *Malignancy* - While malignant pleural effusions (lymphoma, metastatic carcinoma) can present with **lymphocytic predominance** and exudative characteristics, the clinical context is crucial. - The patient's **young age** and presentation in an **endemic area for tuberculosis** makes TB far more likely than malignancy. - In endemic areas, TB should be ruled out first before considering malignancy in young patients with lymphocytic pleural effusions.
Question 8: A patient presents with acute epigastric pain and an increase in serum lipase. Several days after stabilization, a chest X-ray shows bilateral diffuse infiltrates. What is the most common pathology explaining the chest X-ray findings?
- A. Increased PCWP
- B. Pulmonary thromboembolism
- C. Non-cardiogenic pulmonary edema (Correct Answer)
- D. Aspiration pneumonitis
- E. Pleural effusion
Explanation: ***Non-cardiogenic pulmonary edema*** - The patient's presentation with **acute epigastric pain** and **elevated serum lipase** is consistent with **acute pancreatitis**, which is a known cause of **ARDS (acute respiratory distress syndrome)**. - The chest X-ray findings of **bilateral diffuse infiltrates** without signs of cardiomegaly or pleural effusions are characteristic of **non-cardiogenic pulmonary edema** caused by ARDS. - ARDS complicates approximately **10-20% of severe acute pancreatitis cases** and presents with hypoxemia and bilateral pulmonary infiltrates. *Increased PCWP* - **Increased pulmonary capillary wedge pressure (PCWP)** is characteristic of **cardiogenic pulmonary edema**, where a failing heart causes increased pressure in the lungs. - The X-ray findings and clinical context of pancreatitis suggest a **non-cardiac cause** for the pulmonary edema, and PCWP would be **normal or low in ARDS**. *Pulmonary thromboembolism* - **Pulmonary embolism (PE)** often presents with **dyspnea, pleuritic chest pain**, and sometimes **tachycardia** or **hemoptysis**. - Chest X-rays in PE are often **normal** or show subtle findings like **Westermark sign** or **Hampton's hump**, which are not seen here. - The **bilateral diffuse infiltrates** are not typical of PE. *Aspiration pneumonitis* - **Aspiration pneumonitis** typically occurs in patients with impaired consciousness or dysphagia and usually presents with infiltrates in **dependent lung segments**, often the right lower lobe. - While pancreatitis can lead to nausea and vomiting, the **diffuse and bilateral** nature of the infiltrates is less typical for a primary aspiration event. *Pleural effusion* - **Pleural effusions** are a common complication of acute pancreatitis (occurring in up to **20% of cases**), typically left-sided or bilateral. - However, the described chest X-ray findings of **bilateral diffuse infiltrates** represent **parenchymal disease**, not simply fluid in the pleural space. - Pleural effusions would appear as **blunting of costophrenic angles** or fluid layering, not diffuse infiltrates.
Question 9: A patient with a history of hypertension presents with atrial fibrillation, shortness of breath, and bilateral basal crackles on auscultation. Which of the following would be the least important in the management of this patient?
- A. Start on anticoagulants
- B. Start β-blocker
- C. Cardioversion to correct rhythm if hemodynamically remains unstable even after medical management
- D. IV Digoxin for control rate (Correct Answer)
- E. Administer diuretics for fluid overload
Explanation: ***IV Digoxin for control rate*** - While **Digoxin** can be used for **rate control in atrial fibrillation**, its role is limited, especially in patients with **congestive heart failure** due to its delayed onset of action and narrow therapeutic window. - In a patient with **shortness of breath** and **bilateral basal crackles** (suggesting acute decompensated heart failure), rapid rate control with a **β-blocker** or **calcium channel blocker** is usually preferred for immediate symptom relief. - Digoxin is not first-line therapy in this acute setting and is therefore the **least important** among the management options listed. *Start on anticoagulants* - **Anticoagulation** is crucial for patients with **atrial fibrillation** to prevent **thromboembolic events**, particularly strokes. - Given the patient's history of **hypertension** and presence of **atrial fibrillation**, their **CHA2DS2-VASc score** is likely elevated, necessitating anticoagulation. *Start β-blocker* - **Beta-blockers** are first-line agents for **rate control in atrial fibrillation**, especially in patients with **hypertension** and signs of **heart failure**. - They effectively reduce ventricular response rate, improve diastolic filling, and can alleviate symptoms like **shortness of breath**. *Cardioversion to correct rhythm if hemodynamically remains unstable even after medical management* - If a patient with **atrial fibrillation** and signs of **heart failure** remains **hemodynamically unstable** despite initial medical management (e.g., rate control, diuretics), **cardioversion** (electrical or pharmacological) is an essential intervention to restore sinus rhythm. - This can acutely improve cardiac output and resolve symptoms of **decompensated heart failure**. *Administer diuretics for fluid overload* - **Diuretics** (e.g., furosemide) are essential for managing the **volume overload** in this patient, as evidenced by **bilateral basal crackles** and **shortness of breath**. - Reducing preload helps improve **pulmonary congestion** and alleviates acute heart failure symptoms. - Loop diuretics are a cornerstone of acute decompensated heart failure management.
Question 10: In Type 1 Diabetes Mellitus (DM) stage 3 beta cell destruction, which of the following is the most likely presentation?
- A. Dysglycemic symptomatic
- B. Normoglycemic symptomatic
- C. Dysglycemic asymptomatic
- D. Hyperglycemia symptomatic (Correct Answer)
- E. Normoglycemic asymptomatic
Explanation: ***Hyperglycemia symptomatic*** - **Type 1 DM stage 3** is characterized by sufficient **beta-cell destruction** to cause overt hyperglycemia. - This level of hyperglycemia typically leads to classic symptoms such as **polyuria, polydipsia, and weight loss**. *Dysglycemic symptomatic* - **Dysglycemic** refers to abnormal blood sugar levels, but this term is too broad and doesn't specify the degree or symptomatic nature as precisely as **hyperglycemia symptomatic**. - While patients are symptomatic, the primary issue is **hyperglycemia**, making that a more specific and accurate description. *Normoglycemic symptomatic* - **Normoglycemic** implies normal blood sugar levels, which is inconsistent with **Type 1 DM stage 3** where significant beta-cell destruction has occurred. - This stage is defined by definite hyperglycemia, so a patient cannot be symptomatic while having normal glucose levels due to the disease. *Dysglycemic asymptomatic* - While there is **dysglycemia**, **asymptomatic presentation** is more characteristic of earlier stages (Type 1 DM stage 2), where hyperglycemia is present but not yet severe enough to cause overt symptoms. - In **stage 3**, beta-cell destruction is substantial, leading to glucose levels that are high enough to cause noticeable symptoms. *Normoglycemic asymptomatic* - **Normoglycemic asymptomatic** describes **Type 1 DM stage 1**, where autoimmunity is present but beta-cell destruction has not yet progressed enough to affect glucose levels. - This is the earliest stage of Type 1 DM, well before the overt hyperglycemia seen in stage 3.