NEET-PG 2024 — ENT
8 Previous Year Questions with Answers & Explanations
A singer presents with difficulty singing at a high pitch. On examination, bowing of the vocal cord is observed on the right side. Which of the following muscles has likely been compromised?
In a patient with right vestibular neuronitis, what will be the finding on the head impulse test?
A patient presents with conductive hearing loss, pulsatile tinnitus, and a positive Phelps sign. Based on the CT scan image provided, what is the most likely diagnosis?
A patient with chronic nasal obstruction underwent a procedure 3 months ago and now presents with recurrent epistaxis, crusting, and the clinical image showing a septal perforation. What procedure was most likely carried out?
A 14-year-old child with a history of recurrent nasal bleeding has the endoscopic view provided. What is the investigation of choice?
Which sinus drainage is impaired in the following image?
A female patient's pure tone audiometry (PTA) findings show the presence of a Carhart's notch. Which of the following specific clinical signs can be seen in this patient?
A female patient presents with mild conductive hearing loss (CHL) and tinnitus. Based on the pure tone audiometry (PTA) shown in the image, what is the most likely diagnosis?
NEET-PG 2024 - ENT NEET-PG Practice Questions and MCQs
Question 1: A singer presents with difficulty singing at a high pitch. On examination, bowing of the vocal cord is observed on the right side. Which of the following muscles has likely been compromised?
- A. Posterior cricoarytenoid
- B. Lateral cricoarytenoid
- C. Cricothyroid (Correct Answer)
- D. Thyroarytenoid
Explanation: ***Cricothyroid*** - The **cricothyroid muscle** is primarily responsible for **tensioning and elongating the vocal cords**, which is crucial for increasing vocal pitch. - Damage to this muscle or its innervation (superior laryngeal nerve) results in an inability to reach higher pitches and can cause **vocal cord bowing** due to reduced tension. *Posterior cricoarytenoid* - This muscle is the **primary abductor** of the vocal cords, meaning it opens the vocal cords for breathing. - Compromise would lead to difficulty breathing or a paralyzed vocal cord in the adducted position, not bowing with difficulty singing high notes. *Lateral cricoarytenoid* - The **lateral cricoarytenoid muscle** is a **vocal cord adductor** and rotator, bringing the vocal cords together to regulate voice intensity. - Dysfunction typically results in a weak and breathy voice, or difficulty bringing the cords together, not specifically difficulty with high pitch. *Thyroarytenoid* - The **thyroarytenoid muscle** (which includes the vocalis muscle) acts to **relax and shorten the vocal cords**, lowering pitch and modulating vocal cord tension. - Dysfunction would primarily lead to difficulty with lower pitches or a hoarse voice, as it prevents proper relaxation of the vocal cords.
Question 2: In a patient with right vestibular neuronitis, what will be the finding on the head impulse test?
- A. Head turned to right, corrective saccade to the left (Correct Answer)
- B. Head turned to left, corrective saccade to the right
- C. Head turned to right, no corrective saccade
- D. Head turned to left, no corrective saccade
Explanation: ***Head turned to right, corrective saccade to the left*** - In **right vestibular neuronitis**, the right vestibular apparatus is impaired, affecting the **vestibulo-ocular reflex (VOR)** on that side. - During the head impulse test, when the head is rapidly turned **to the right** (toward the affected side), the impaired VOR cannot maintain eye fixation on the target. - The eyes initially move **with the head** (to the right), then a visible **corrective saccade** (catch-up saccade) brings them **back to the left** to refixate on the target. - This corrective saccade is the **hallmark positive finding** in head impulse test for right vestibular dysfunction. *Head turned to left, corrective saccade to the right* - This would indicate a **left vestibular lesion**, not right vestibular neuronitis. - When turning the head to the left with left vestibular dysfunction, a corrective saccade to the right would be observed. *Head turned to right, no corrective saccade* - This would indicate **normal VOR function** on the right side. - A normal response shows no corrective saccade because the eyes maintain fixation throughout the head turn. - This is the **opposite** of what is expected in right vestibular neuronitis. *Head turned to left, no corrective saccade* - This indicates normal VOR function on the left side. - In right vestibular neuronitis, turning the head to the left (away from the affected side) typically shows **normal VOR** with no corrective saccade needed.
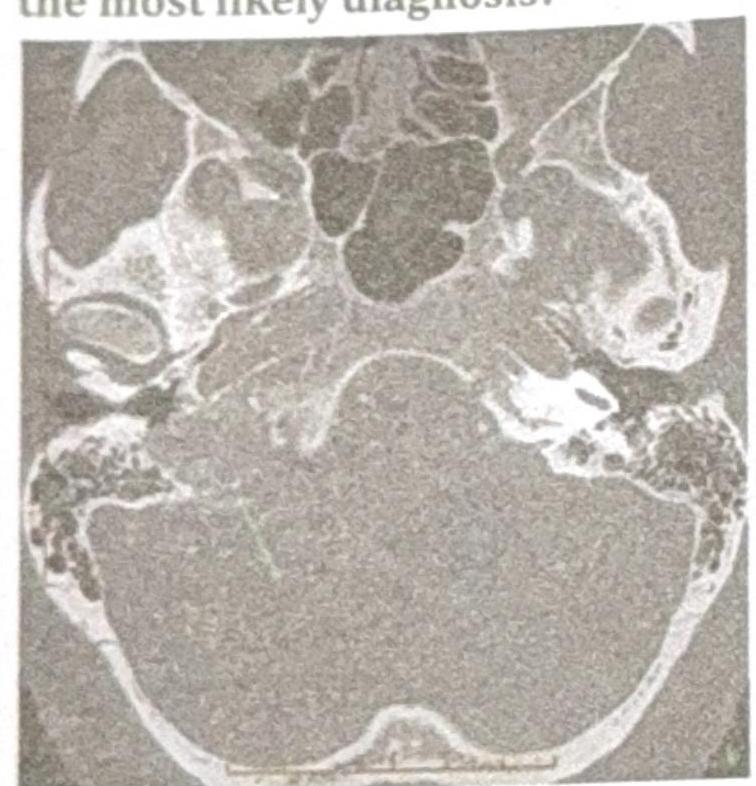
Question 3: A patient presents with conductive hearing loss, pulsatile tinnitus, and a positive Phelps sign. Based on the CT scan image provided, what is the most likely diagnosis?
- A. Glomus Jugulare (Correct Answer)
- B. Glomus Tympanicum
- C. Acoustic Neuroma
- D. Cholesteatoma
Explanation: ***Glomus Jugulare*** - The symptoms of **conductive hearing loss**, **pulsatile tinnitus**, and a **positive Phelps sign** (destruction of the bone separating the carotid artery from the jugular bulb on CT) are classic for a glomus jugulare tumor. - The CT scan image, showing a destructive lesion in the **jugular foramen** region, further supports this diagnosis, as these tumors originate from the paraganglia of the jugular bulb. *Glomus Tympanicum* - While it can cause conductive hearing loss and pulsatile tinnitus, a glomus tympanicum tumor is typically **confined to the middle ear cavity** and does not involve bone erosion of the jugular foramen as indicated by a positive Phelps sign. - The CT findings would show a mass in the middle ear, often behind an intact tympanic membrane, rather than extensive bone destruction in the jugular region. *Acoustic Neuroma* - This tumor, also known as a **vestibular schwannoma**, primarily causes **sensorineural hearing loss**, **tinnitus** (often non-pulsatile), and **balance issues**, not conductive hearing loss or pulsatile tinnitus. - An acoustic neuroma is located in the **cerebellopontine angle** and internal auditory canal, and the CT scan would show a mass in this specific location, not necessarily bone erosion of the jugular foramen. *Cholesteatoma* - A cholesteatoma is a **destructive, expanding growth of keratinizing squamous epithelium** in the middle ear or mastoid, typically presenting with **conductive hearing loss**, **otorrhea**, and sometimes headaches. - It does not typically cause pulsatile tinnitus unless it's very large and vascularized, nor does it present with the characteristic destruction of the jugular foramen seen with a positive Phelps sign.
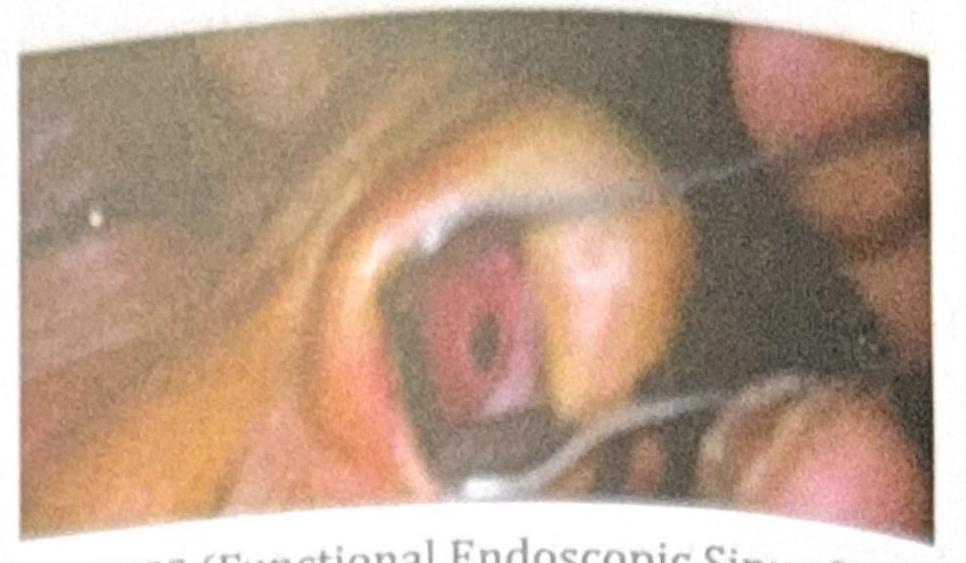
Question 4: A patient with chronic nasal obstruction underwent a procedure 3 months ago and now presents with recurrent epistaxis, crusting, and the clinical image showing a septal perforation. What procedure was most likely carried out?
- A. FESS (Functional Endoscopic Sinus Surgery)
- B. Caldwell-Luc's procedure
- C. Submucosal resection (SMR) (Correct Answer)
- D. Turbinate reduction surgery
Explanation: ***Submucosal resection (SMR)*** - **SMR** involves removing cartilage or bone from the nasal septum while preserving the septal mucosa. If both mucosal flaps are inadvertently damaged or devitalized during the procedure, it can lead to a **septal perforation** as a complication. - The symptoms of **recurrent epistaxis** and **crusting** are classic signs associated with compromised septal integrity and airflow changes due to a septal perforation, which commonly occurs weeks to months after such a procedure. *FESS (Functional Endoscopic Sinus Surgery)* - **FESS** is primarily used to treat chronic sinusitis by opening and ventilating the sinuses; it does not directly involve the nasal septum in a way that typically causes perforation. - While complications are possible, a septal perforation is not a common or direct consequence of FESS, which focuses on ethmoid, maxillary, frontal, or sphenoid sinus drainage pathways. *Caldwell-Luc's procedure* - The **Caldwell-Luc procedure** involves an incision above the canine fossa to access the maxillary sinus. - It is specifically aimed at the maxillary sinus and does not involve surgical manipulation of the nasal septum that would lead to a septal perforation. *Turbinate reduction surgery* - **Turbinate reduction** procedures target the inferior turbinates to improve nasal airflow by reducing their size. - These procedures do not involve the nasal septum itself, so a septal perforation would not be a direct or common complication.
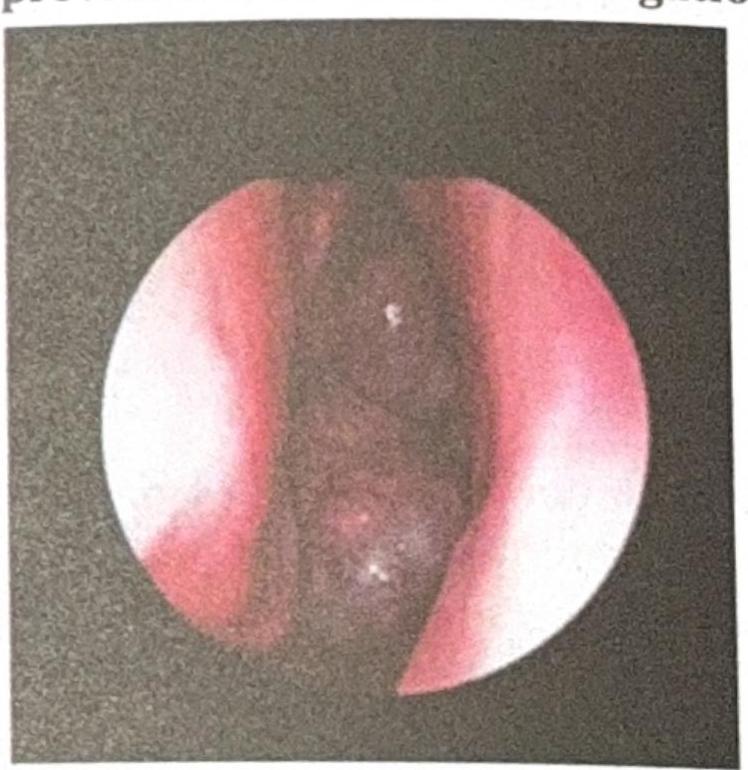
Question 5: A 14-year-old child with a history of recurrent nasal bleeding has the endoscopic view provided. What is the investigation of choice?
- A. Biopsy
- B. X-ray
- C. FESS (Functional Endoscopic Sinus Surgery)
- D. CECT (Contrast-Enhanced CT) (Correct Answer)
Explanation: ***CECT (Contrast-Enhanced CT)*** - Given the history of recurrent nasal bleeding in an adolescent male suggestive of a **juvenile nasopharyngeal angiofibroma (JNA)**, CECT is the investigation of choice to delineate the tumor's extent, vascularity, and involvement of surrounding structures. - CECT provides crucial information for surgical planning and assessing intracranial extension due to the highly vascular nature of JNAs. *Biopsy* - Biopsy of a suspected angiofibroma is generally **contraindicated** due to the high risk of severe and uncontrolled hemorrhage because the tumor is highly vascular and lacks a true capsule. - The diagnosis of JNA is usually made based on clinical presentation and imaging findings. *X-ray* - **X-rays** (like plain radiographs of the sinuses) offer limited soft tissue detail and are **insufficient** to accurately visualize the extent or vascularity of a nasopharyngeal mass. - They may show some bony erosion but cannot provide the detailed information needed for diagnosis or surgical planning of a JNA. *FESS (Functional Endoscopic Sinus Surgery)* - **FESS** is a **surgical procedure** used for treating chronic sinusitis and other sinonasal conditions, not primarily an investigative tool for a suspected tumor like JNA. - While endoscopy is used for initial visualization, **surgery** is a treatment, and detailed imaging must precede it to understand tumor boundaries.
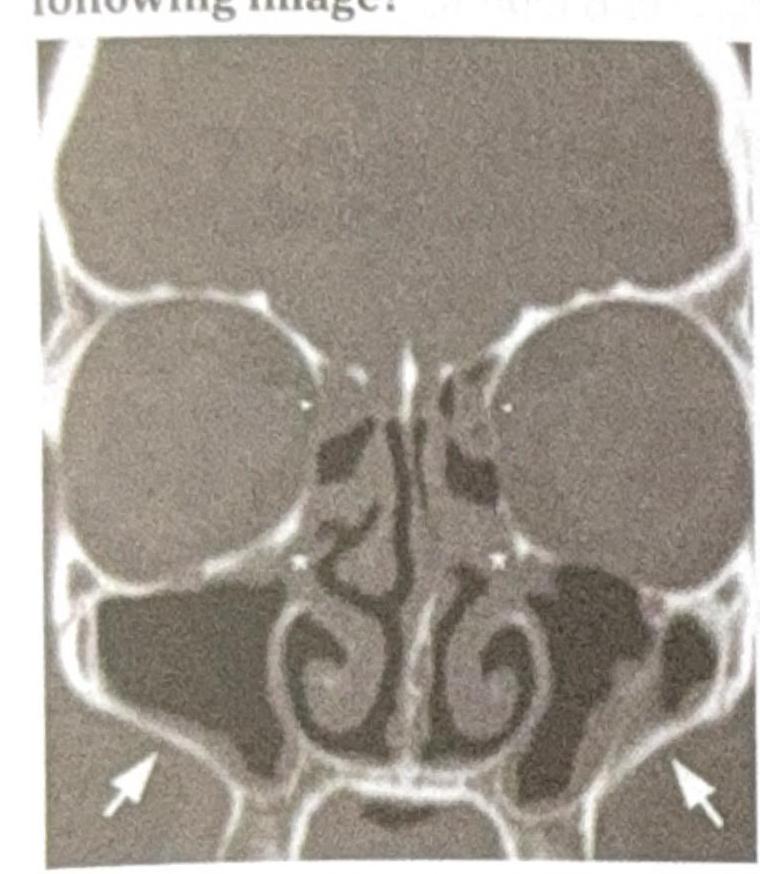
Question 6: Which sinus drainage is impaired in the following image?
- A. Ethmoid
- B. Sphenoid
- C. Frontal
- D. Maxillary (Correct Answer)
Explanation: ***Maxillary*** - The image shows **arrows pointing to the maxillary sinuses** with visible **opacification and fluid accumulation**, indicating **impaired drainage**. - Maxillary sinuses drain through the **ostiomeatal complex** into the middle meatus; obstruction leads to mucus retention and sinusitis. *Ethmoid* - The **ethmoid air cells** located between the eyes, medial to the orbits, do not show significant **opacification** or drainage impairment. - These complex honeycomb-like structures appear **relatively clear** without evidence of fluid accumulation. *Sphenoid* - The **sphenoid sinuses** located deeper in the skull, behind the ethmoid sinuses, are **not prominently affected** in this image. - No significant **opacification** or mucosal thickening visible to suggest impaired drainage. *Frontal* - The **frontal sinuses** located above the eyebrows appear **relatively clear** without significant opacification or drainage impairment. - These sinuses drain through the **frontonasal duct** and do not show evidence of fluid retention in this image.
Question 7: A female patient's pure tone audiometry (PTA) findings show the presence of a Carhart's notch. Which of the following specific clinical signs can be seen in this patient?
- A. Schwartz sign (Correct Answer)
- B. Hitselberger sign
- C. Hennebert sign
- D. Rinne test negative (conductive hearing loss)
Explanation: ***Schwartz sign*** - A **Carhart's notch** (bone conduction dip at 2000 Hz) is a characteristic finding in **otosclerosis**, a condition where the stapes bone becomes fixed. - The **Schwartz sign** (reddish/pinkish hue behind the tympanic membrane) indicates **active otosclerosis** with increased vascularity in the promontory. - This is a **specific clinical sign** directly associated with otosclerosis and would be the expected finding on otoscopy. *Hitselberger sign* - The **Hitselberger sign** refers to **hypesthesia** (numbness or decreased sensation) in the **posterior external auditory canal wall**. - It is associated with **acoustic neuromas** (vestibular schwannomas) due to compression of the facial nerve, not otosclerosis. *Hennebert sign* - The **Hennebert sign** involves **nystagmus or vertigo** induced by changes in external ear canal pressure (fistula test). - It is typically seen in conditions causing a **perilymphatic fistula**, such as **Meniere's disease** or **syphilitic labyrinthitis**, not otosclerosis. *Rinne test negative (conductive hearing loss)* - While otosclerosis does cause **conductive hearing loss** with a negative Rinne test (bone conduction > air conduction), this is a **general audiometric finding**, not a specific clinical sign. - A negative Rinne test can occur in **any cause of conductive hearing loss** (chronic otitis media, ossicular discontinuity, cholesteatoma, etc.). - The question asks for a **specific clinical sign**, making the **Schwartz sign** the most appropriate answer as it specifically indicates otosclerosis.
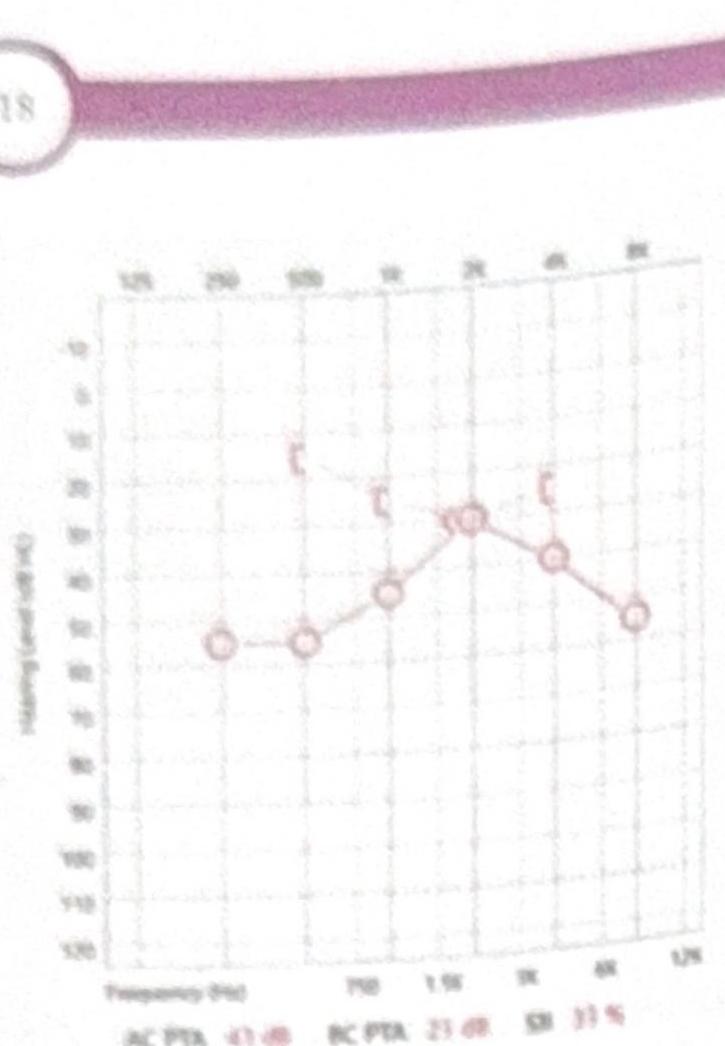
Question 8: A female patient presents with mild conductive hearing loss (CHL) and tinnitus. Based on the pure tone audiometry (PTA) shown in the image, what is the most likely diagnosis?
- A. Ménière's disease
- B. Otosclerosis (Correct Answer)
- C. Ototoxicity
- D. Noise-Induced Hearing Loss (NIHL)
Explanation: ***Otosclerosis*** - The audiogram shows a **conductive hearing loss** with a notable **Carhart notch** (bone conduction dip at 2000 Hz), which is characteristic of otosclerosis. - The patient's symptoms of **mild CHL** and **tinnitus** are consistent with the presentation of otosclerosis, a condition involving abnormal bone growth in the middle ear. *Ménière's disease* - This condition primarily causes **sensorineural hearing loss**, often fluctuating and affecting low frequencies initially, along with **vertigo, tinnitus, and aural fullness**. - The audiogram indicates **conductive hearing loss**, not sensorineural, and **vertigo** is not mentioned as a primary symptom. *Ototoxicity* - Ototoxicity typically results in **sensorineural hearing loss**, often bilateral and affecting high frequencies first. - The audiogram demonstrates **conductive hearing loss**, and there is no information about exposure to ototoxic medications. *Noise-Induced Hearing Loss (NIHL)* - NIHL is characterized by **sensorineural hearing loss**, typically with a **notch at 3000-6000 Hz** (most commonly 4000 Hz notch) on the audiogram. - The audiogram reflects **conductive hearing loss**, and the specific pattern does not match that of NIHL.