NEET-PG 2024 — Diagnosis
3 Previous Year Questions with Answers & Explanations
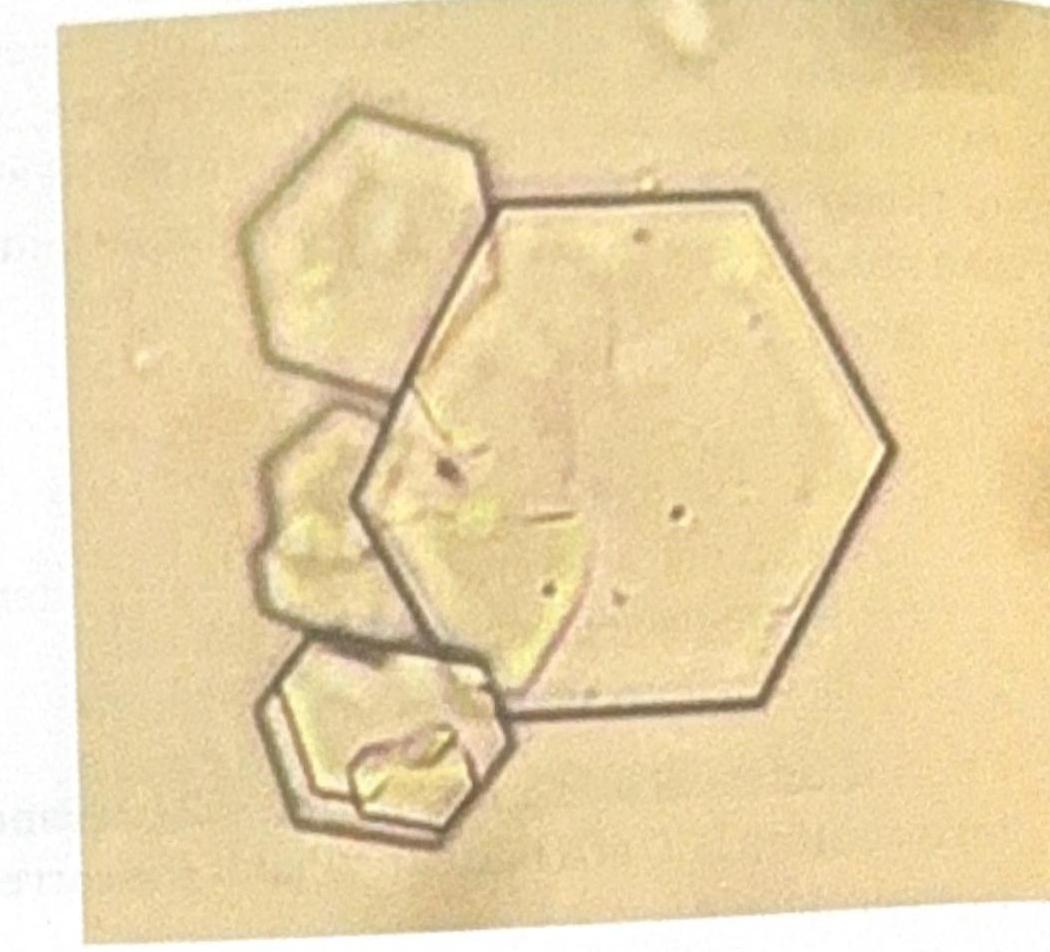
A young patient presents to the OPD with recurrent colicky abdominal pain. Urine examination shows the presence of red blood cells (RBCs) and the following crystal shape in the figure. What is the most likely diagnosis?
What is the most appropriate initial investigation for a solitary thyroid nodule (STN)?
A female presents with a 1 × 1 cm thyroid swelling. What is the next best step in management?
NEET-PG 2024 - Diagnosis NEET-PG Practice Questions and MCQs
Question 1: A young patient presents to the OPD with recurrent colicky abdominal pain. Urine examination shows the presence of red blood cells (RBCs) and the following crystal shape in the figure. What is the most likely diagnosis?
- A. Cystine stone (Correct Answer)
- B. Glomerulonephritis
- C. Oxalate stone
- D. Polycystic kidney disease
- E. Uric acid stone
Explanation: ***Cystine stone*** - The image displays classic **hexagonal** crystals, which are pathognomonic for **cystine stones**. - Recurrent colicky abdominal pain in a young patient with hematuria (RBCs in urine) is highly suggestive of **nephrolithiasis** (kidney stones), and the crystal morphology confirms cystine as the cause. - Cystine stones are associated with **cystinuria**, an autosomal recessive disorder causing defective renal tubular reabsorption of cystine. *Glomerulonephritis* - While glomerulonephritis can cause hematuria, the presence of **hexagonal crystals** in the urine is not a feature of this condition. - Glomerulonephritis typically involves **dysmorphic RBCs** and **RBC casts** in the urine, not hexagonal crystals. *Oxalate stone* - **Calcium oxalate crystals** typically appear as **envelope-shaped (dihydrate)** or **dumbbell-shaped (monohydrate)**. - While oxalate stones are the most common cause of kidney stones and colicky pain, their crystal morphology is distinct from the hexagonal shape seen here. *Polycystic kidney disease* - Polycystic kidney disease is a genetic disorder characterized by **multiple cysts** in the kidneys, which can cause pain and hematuria. - However, it does **not** typically present with specific crystal shapes like those shown in the image, as the primary pathology is structural, not related to crystal formation. *Uric acid stone* - **Uric acid crystals** typically appear as **rhomboid or diamond-shaped** crystals, often with a yellow-brown color. - While uric acid stones can cause similar symptoms (colicky pain, hematuria), the crystal morphology is distinctly different from the hexagonal cystine crystals shown in the image. - Uric acid stones are associated with **hyperuricemia**, **low urine pH**, and conditions like gout.
Question 2: What is the most appropriate initial investigation for a solitary thyroid nodule (STN)?
- A. I-123 scan
- B. Ultrasound (Correct Answer)
- C. Fine-needle aspiration (FNA) biopsy
- D. Thyroid function tests (TFTs)
- E. CT scan of the neck
Explanation: ***Ultrasound*** - **Ultrasound** is the initial investigation of choice for a solitary thyroid nodule (STN) because it can differentiate between **solid, cystic, or mixed lesions**, assess nodule size, and identify suspicious features (e.g., microcalcifications, irregular margins, internal vascularity). - It also helps to determine if there are other nodules not palpable on physical examination, allowing for a more complete assessment of the **thyroid gland**. *Fine-needle aspiration (FNA) biopsy* - **FNA biopsy** is the most accurate diagnostic tool for evaluating the malignant potential of a thyroid nodule, but it is typically performed *after* an initial ultrasound has characterized the nodule. - It requires guidance (often by ultrasound) to obtain an adequate sample for cytological analysis, making ultrasound a prerequisite for optimal FNA performance. *Thyroid function tests (TFTs)* - **TFTs (TSH, T3, T4)** are important for assessing the functional status of the thyroid gland (e.g., hyperthyroidism or hypothyroidism) and can provide context for the nodule. - However, TFTs do not directly evaluate the **morphology or malignant potential** of the nodule itself, making them less appropriate as an initial, stand-alone investigation for an STN. *I-123 scan* - An **I-123 scan** (radioactive iodine uptake and scan) is used to determine if a nodule is "hot" (hyperfunctioning/benign) or "cold" (non-functioning/potentially malignant). - It is typically reserved for cases where **TSH levels are suppressed**, suggesting a hyperfunctioning nodule, and is not the first-line imaging modality for initial characterization of all STNs. *CT scan of the neck* - **CT scan** can visualize thyroid nodules and assess for extrathyroidal extension or lymphadenopathy, but it is **not recommended as an initial investigation** for STN. - It involves **radiation exposure**, is more expensive than ultrasound, and provides **less detailed characterization** of nodule morphology compared to ultrasound, making it a less appropriate first-line modality.
Question 3: A female presents with a 1 × 1 cm thyroid swelling. What is the next best step in management?
- A. I-131
- B. TSH (Correct Answer)
- C. TSH & T4
- D. T3 & T4
- E. FNAC
Explanation: ***Correct Option: TSH*** - **Thyroid-stimulating hormone (TSH)** is the most sensitive initial test to assess thyroid function when a thyroid nodule is discovered. - An abnormal TSH level (either high or low) can guide further investigation into whether the nodule is associated with a functional thyroid disorder. - **TSH should be the first test** according to American Thyroid Association guidelines for thyroid nodule evaluation. *Incorrect Option: I-131* - **I-131 (radioactive iodine therapy)** is a treatment modality for hyperthyroidism or thyroid cancer, not a diagnostic step for initial thyroid swelling evaluation. - Administering I-131 before assessing thyroid function would be inappropriate and could lead to unnecessary or harmful intervention. *Incorrect Option: TSH & T4* - While TSH is crucial, adding **T4 (thyroxine)** as an initial step is often not necessary if TSH is normal, as TSH alone effectively screens for primary thyroid dysfunction. - Measuring both TSH and T4 is typically reserved for situations where TSH is abnormal or when central hypothyroidism is suspected. *Incorrect Option: T3 & T4* - Measuring **T3 (triiodothyronine)** along with T4 as an initial screening for a thyroid nodule is generally not recommended. - T3 levels are primarily used to diagnose **hyperthyroidism** or to evaluate the severity of thyrotoxicosis after an abnormal TSH and T4 have been identified. *Incorrect Option: FNAC* - While **Fine Needle Aspiration Cytology (FNAC)** is an essential diagnostic tool for thyroid nodules, it is typically performed after TSH assessment. - FNAC is indicated for nodules >1 cm with suspicious ultrasound features, but **functional assessment with TSH comes first** to rule out hyperfunctioning nodules.