NEET-PG 2024 — Dermatology
11 Previous Year Questions with Answers & Explanations
A patient who has always neglected his nutrition presented with follicular hyperkeratosis on the extensor aspect of the forearm. What is the diagnosis?
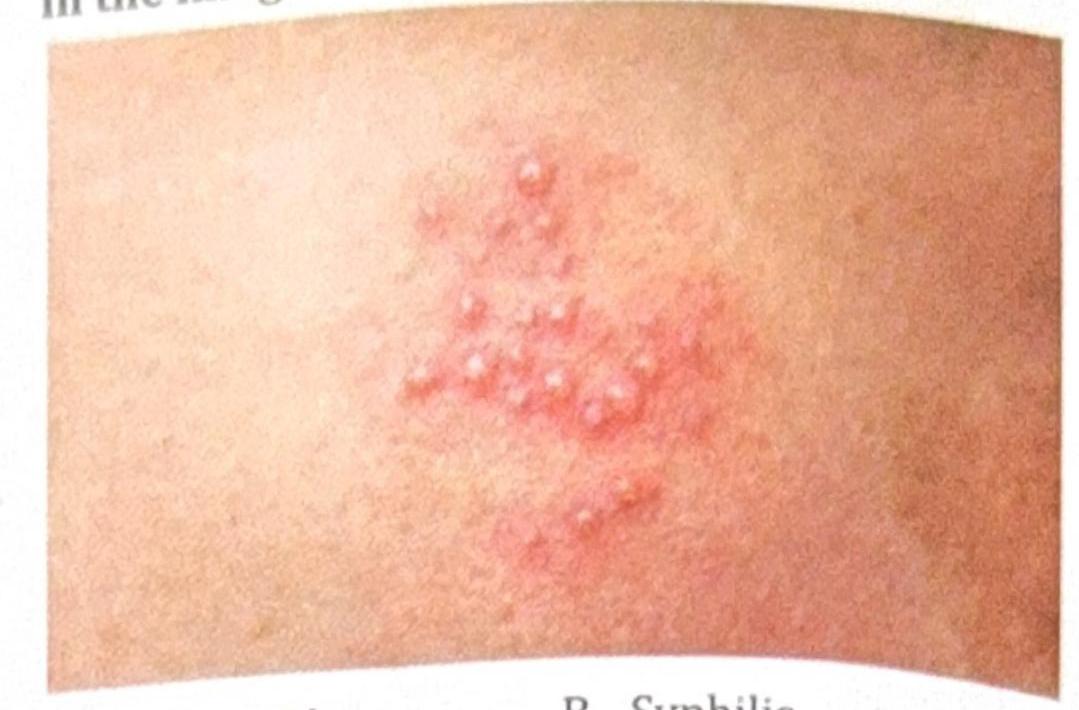
A patient presents with painful vesicles as shown in the image. What is the diagnosis?
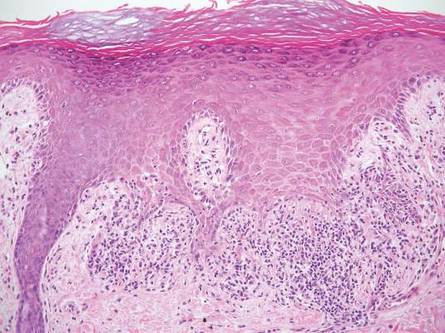
The skin biopsy shown below is most consistent with which of the following conditions? 
A child presents with itchy lesions and diarrhea and has been advised to follow a gluten-free diet. What is the most likely etiology of this condition?
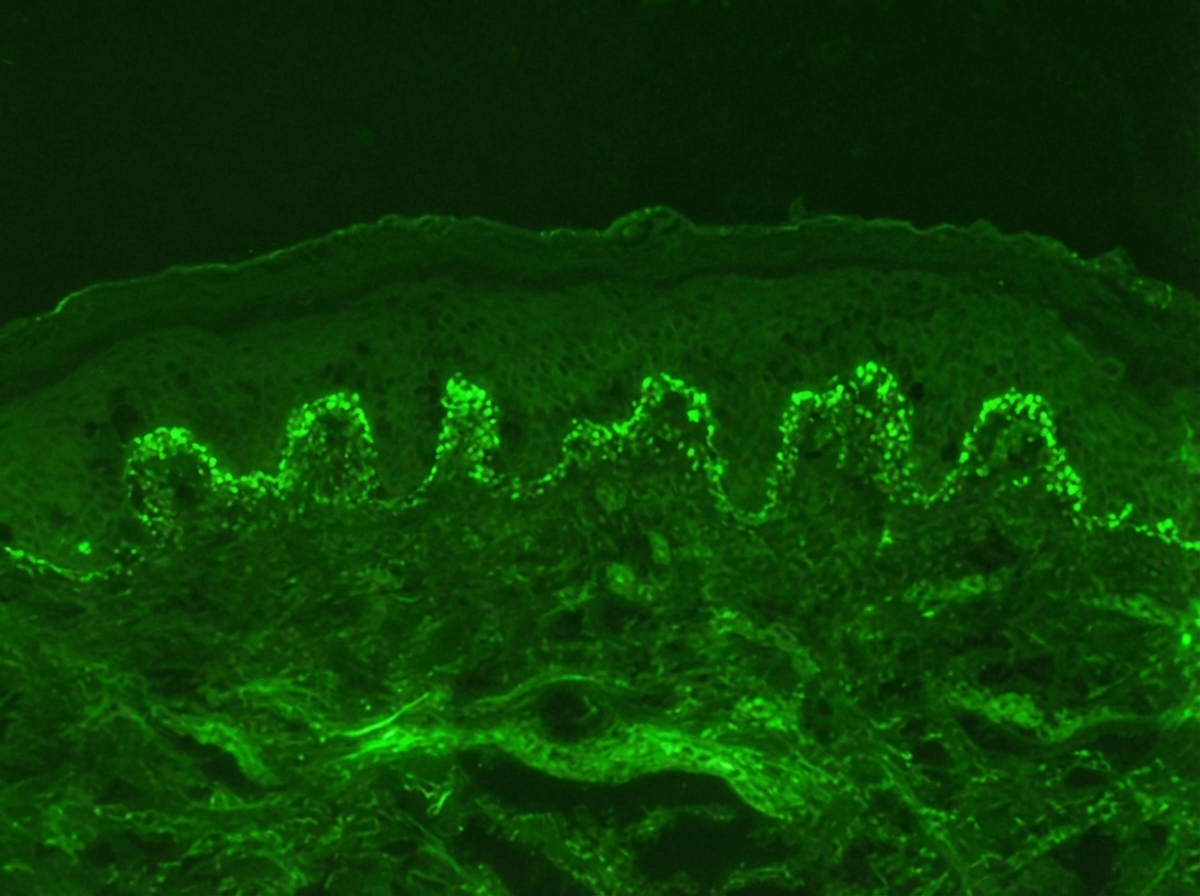
Identify the diagnosis based on the dermatology immunofluorescence (IF) image provided.
A patient's skin biopsy shows a box-shaped or square-shaped pattern of inflammatory infiltrate, as shown in the image. What is the most likely diagnosis?
A patient presents with orange-hued skin lesions and hyperkeratotic palms and soles. A biopsy shows alternating parakeratosis and orthokeratosis. What is the most likely diagnosis?
A patient presents with annular, scaly plaques with perifollicular extension on the trunk. What is the most likely diagnosis?
An adolescent male presents with severe acne lesions and sinus tracts. Which is the most effective drug for this condition?
A patient presents with skin lesions and erosions on the buccal mucosa. The immunofluorescence image is shown. What is the most likely diagnosis?
NEET-PG 2024 - Dermatology NEET-PG Practice Questions and MCQs
Question 1: A patient who has always neglected his nutrition presented with follicular hyperkeratosis on the extensor aspect of the forearm. What is the diagnosis?
- A. Phrynoderma (Correct Answer)
- B. Eruptive xanthoma
- C. Darier's disease
- D. Folliculitis
Explanation: ***Phrynoderma*** - **Phrynoderma**, also known as **toad skin**, is characterized by **follicular hyperkeratosis**, particularly on the **extensor surfaces** of limbs like the forearm. - This condition is closely linked to **nutritional deficiencies**, often involving **vitamin A**, **essential fatty acids**, or sometimes **B vitamins**. *Eruptive xanthoma* - **Eruptive xanthomas** are small, yellow-red papules that often appear suddenly, typically on the **buttocks**, **extensor surfaces of the limbs**, and **trunk**. - They are a cutaneous manifestation of **severe hypertriglyceridemia** and not primarily related to general nutritional neglect or follicular hyperkeratosis. *Darier's disease* - **Darier's disease** is a **rare, inherited genetic disorder** characterized by greasy, crusted papules primarily in **seborrheic areas** such as the scalp, forehead, chest, and groin. - It results from a mutation in the **ATP2A2 gene**, affecting calcium signaling in keratinocytes, and is not a nutritional deficiency condition. *Folliculitis* - **Folliculitis** is the inflammation of one or more **hair follicles**, often caused by **bacterial** (e.g., *Staphylococcus aureus*) or **fungal infections**. - It presents as small, red, sometimes pus-filled bumps around hair follicles, distinct from the dry, rough texture of follicular hyperkeratosis seen in phrynoderma.
Question 2: A patient presents with painful vesicles as shown in the image. What is the diagnosis?
- A. Chancroid
- B. Syphilis
- C. Herpes (Correct Answer)
- D. Candidiasis
Explanation: ***Herpes*** - The image shows a cluster of **small, painful vesicles on an erythematous base**, which is highly characteristic of a herpes simplex virus (HSV) infection. - These lesions typically evolve into ulcers, crust over, and heal, and are often recurrent. *Chancroid* - Chancroid presents as **painful, soft chancres** (ulcers) with irregular, undermined borders and a gray or yellow base, often accompanied by **buboes** (enlarged, tender lymph nodes). - It does not typically manifest as clusters of small vesicles. *Syphilis* - Primary syphilis presents as a **painless chancre**—a single, firm, ulcerated lesion with a clean base and raised borders. - Secondary syphilis can cause a variety of skin manifestations, but not painful vesicles. *Candidiasis* - Cutaneous candidiasis usually appears as a **red, moist rash with satellite lesions** (smaller papules or pustules spreading from the main rash), often in skin folds. - While it can be inflammatory and itchy, it does not typically form discreet painful vesicles as seen in the image.
Question 3: The skin biopsy shown below is most consistent with which of the following conditions? 
- A. Lichen planus (Correct Answer)
- B. Lichen nitidus
- C. Morphea
- D. Lupus erythematosus
Explanation: ***Lichen planus*** - The image shows **basal cell degeneration** (liquefaction degeneration), a **sawtooth rete ridge pattern**, and a band-like inflammatory infiltrate primarily composed of lymphocytes at the dermo-epidermal junction, which are classic histological features of **lichen planus**. - **Civatte bodies** (apoptotic keratinocytes forming colloid bodies) are typically present, resulting from keratinocyte damage at the basal layer. - These features make lichen planus the most consistent diagnosis. *Lichen nitidus* - Characterized by **"ball and claw" lesions**, which are small, localized epidermal invaginations enclosing a central infiltrate of lymphocytes and histiocytes. - The granulomatous infiltrate is more focal and circumscribed compared to the band-like pattern of lichen planus. - While both are interface dermatitides, the architectural pattern differs significantly. *Morphea* - This is a localized form of **scleroderma**, characterized by increased **collagen deposition**, thickening of the dermis, and loss of adnexal structures like hair follicles and sweat glands. - The inflammatory infiltrate is typically perivascular and interstitial, not band-like at the dermo-epidermal junction. - The image does not show features of dermal fibrosis or homogenization of collagen bundles expected in morphea. *Lupus erythematosus* - Also shows **interface dermatitis** with basal vacuolar changes and lymphocytic infiltrate. - However, lupus typically shows a **perivascular and periappendageal pattern** of infiltrate rather than the dense band-like pattern of lichen planus. - Additional features in lupus include dermal mucin deposition, thickened basement membrane (PAS-positive), and follicular plugging. - The dense, continuous band-like infiltrate and sawtooth rete ridges favor lichen planus over lupus.
Question 4: A child presents with itchy lesions and diarrhea and has been advised to follow a gluten-free diet. What is the most likely etiology of this condition?
- A. Whipple's disease
- B. Crohn's disease
- C. Dermatitis herpetiformis
- D. Celiac disease (Correct Answer)
Explanation: ***Celiac disease*** - **Celiac disease** is an autoimmune condition triggered by **gluten ingestion**, leading to small intestine damage and nutrient malabsorption. - The combination of **itchy lesions** (dermatitis herpetiformis, a skin manifestation of celiac disease), **diarrhea**, and improvement on a **gluten-free diet** are highly characteristic. - Since the question asks for the **underlying etiology**, celiac disease is the correct answer as it causes both the skin and GI manifestations. *Whipple's disease* - This is a rare systemic infection caused by the bacterium **Tropheryma whipplei**, presenting with **arthralgia, fever, malabsorption, and lymphadenopathy**. - While it can cause diarrhea and malabsorption, it is not associated with itchy skin lesions and does not respond to a gluten-free diet. *Crohn's disease* - **Crohn's disease** is a type of inflammatory bowel disease affecting any part of the GI tract, causing **abdominal pain, diarrhea, and weight loss**. - It is not associated with dermatitis herpetiformis and does not improve with a gluten-free diet (though some patients may have gluten sensitivity). *Dermatitis herpetiformis* - **Dermatitis herpetiformis** is the **cutaneous manifestation of celiac disease**, presenting as intensely itchy, vesicular lesions. - While DH explains the itchy lesions in this case, it is a **symptom/manifestation**, not the underlying **etiology**—the root cause is celiac disease itself, which produces both the intestinal damage (diarrhea) and the skin manifestations (DH).
Question 5: Identify the diagnosis based on the dermatology immunofluorescence (IF) image provided.
- A. Pemphigus vulgaris
- B. Pemphigus foliaceus
- C. Bullous pemphigoid
- D. Dermatitis herpetiformis (Correct Answer)
Explanation: ***Dermatitis herpetiformis*** - The immunofluorescence image shows **granular IgA deposits** at the **dermal papillae region**, which is characteristic of dermatitis herpetiformis. - This condition is strongly associated with **celiac disease** and presents with intensely pruritic papules and vesicles. *Pemphigus vulgaris* - Immunofluorescence in pemphigus vulgaris typically shows a **fishnet pattern** of IgG deposits throughout the **epidermis**, reflecting antibodies against desmoglein 3 and 1. - This pattern is an intercellular deposition, not granular at the dermal papillae. *Pemphigus foliaceus* - Similar to pemphigus vulgaris, pemphigus foliaceus also exhibits **intercellular IgG deposits** in the epidermis, but it is usually more superficial, targeting desmoglein 1. - The image does not show this intercellular epidermal staining. *Bullous pemphigoid* - Bullous pemphigoid is characterized by **linear IgG and C3 deposits along the dermal-epidermal junction** (basement membrane zone). - The image distinctly shows granular IgA, not linear IgG/C3, and specifically in the dermal papillae.
Question 6: A patient's skin biopsy shows a box-shaped or square-shaped pattern of inflammatory infiltrate, as shown in the image. What is the most likely diagnosis?
- A. Lichen planus (Correct Answer)
- B. Lichen amyloidosis
- C. Morphea
- D. Lichen nitidus
Explanation: ***Lichen planus*** - The image shows a characteristic **"box-shaped" or "square-shaped" infiltrate** of lymphocytes at the dermal-epidermal junction, obscuring the basal layer. - Other features consistent with lichen planus include **hypergranulosis**, **sawtooth rete ridges**, and **Civatte bodies** (apoptotic keratinocytes) in the basal layer. *Lichen amyloidosis* - This condition is characterized by deposition of **amyloid material** in the papillary dermis, often associated with keratinocyte necrosis. - While it can present with pruritic papules similar to lichen planus, the histology specifically shows **amyloid deposits**, not the typical basal cell damage or band-like infiltrate seen in the image. *Morphea* - Morphea is a form of localized scleroderma, characterized by **thickening of collagen bundles** in the dermis and subcutaneous tissue, leading to hardened skin plaques. - Histologically, it involves **sclerosis** and homogenization of collagen, with a sparse inflammatory infiltrate, which is distinct from the dense band-like infiltrate and epidermal changes shown. *Lichen nitidus* - Lichen nitidus is characterized by **small, discrete granulomas** within the papillary dermis (the "ball-and-claw" appearance), with epithelial extensions embracing the inflammatory infiltrate. - It involves a more **localized inflammatory process** and distinct granulomatous appearance, rather than the broad, band-like infiltrate seen across the dermal-epidermal junction in this image.
Question 7: A patient presents with orange-hued skin lesions and hyperkeratotic palms and soles. A biopsy shows alternating parakeratosis and orthokeratosis. What is the most likely diagnosis?
- A. Pityriasis rubra pilaris (Correct Answer)
- B. Follicular psoriasis
- C. Keratosis follicularis
- D. Ichthyosis vulgaris
Explanation: ***Pityriasis rubra pilaris*** - This condition classically presents with **salmon-colored to orange-hued plaques** and **hyperkeratotic palms and soles**. - Histologically, Pityriasis rubra pilaris is characterized by **alternating parakeratosis and orthokeratosis** in vertical and horizontal directions ("checkerboard" pattern). *Follicular psoriasis* - While psoriasis can present with hyperkeratosis and scales, **follicular psoriasis** specifically involves the hair follicles, seen as follicular papules and pustules. - The classic alternating parakeratosis and orthokeratosis is more indicative of PRP than of follicular psoriasis, which typically shows more uniform parakeratosis. *Keratosis follicularis* - Also known as Darier disease, this condition presents with **greasy, crusted, foul-smelling papules** on seborrheic areas. - Histopathology reveals characteristic **dyskeratosis** with acantholytic cells (corps ronds and grains), which is different from the described alternating parakeratosis and orthokeratosis. *Ichthyosis vulgaris* - This is a genetic disorder characterized by **dry, scaly skin** due to impaired epidermal barrier function, often worse in winter. - Histopathology typically shows a **diminished or absent granular layer** and compact orthokeratosis without parakeratosis, differing from the biopsy findings.
Question 8: A patient presents with annular, scaly plaques with perifollicular extension on the trunk. What is the most likely diagnosis?
- A. Psoriasis
- B. Lichen planus
- C. Tinea (Correct Answer)
- D. Pityriasis versicolor
Explanation: ***Tinea*** - **Tinea corporis** classically presents with **annular, scaly plaques with central clearing** and an active, raised border. - On hairy areas or with follicular involvement, dermatophyte infections show **perifollicular extension** as the fungus invades hair follicles. - The **annular morphology with scale** is pathognomonic for dermatophyte infection, confirmed by **KOH preparation** showing septate hyphae. - Common sites include trunk, limbs, and any body area with hair follicles. *Psoriasis* - Presents with **well-demarcated, erythematous plaques** with **silvery-white scales**, typically on extensor surfaces (elbows, knees, scalp). - **Follicular psoriasis** is rare and shows **pinpoint follicular papules**, not annular plaques with perifollicular extension. - Auspitz sign (pinpoint bleeding on scale removal) helps differentiate from tinea. *Lichen planus* - Characterized by **pruritic, polygonal, purple, planar papules** (the "6 Ps"). - **Lichen planopilaris** (follicular variant) causes **scarring alopecia** with follicular hyperkeratosis, not annular scaly plaques. - Wickham striae may be visible on mucosal surfaces. *Pityriasis versicolor* - Caused by **Malassezia species**, presents as **hypo- or hyperpigmented macules** with fine scale on trunk and upper arms. - **Follicular variant** (pityriasis folliculorum) shows discrete follicular papules, NOT annular plaques. - "Spaghetti and meatballs" appearance on KOH prep (short hyphae and spores) differentiates from dermatophytes.
Question 9: An adolescent male presents with severe acne lesions and sinus tracts. Which is the most effective drug for this condition?
- A. Minocycline
- B. Doxycycline
- C. Isotretinoin (Correct Answer)
- D. Topical dapsone
Explanation: ***Isotretinoin*** - This patient presents with **severe acne**, likely cystic or nodular, given the mention of "sinus tracts," which often correlates with **acne conglobata**. - **Isotretinoin** is the most effective treatment for severe acne as it targets all four pathogenic factors of acne: **sebaceous gland activity**, **follicular hyperkeratinization**, *C. acnes* proliferation, and inflammation. *Minocycline* - Minocycline is an **oral antibiotic** used for moderate to severe inflammatory acne, primarily due to its anti-inflammatory properties and ability to reduce *C. acnes*. - While effective for some inflammatory acne, it is **less effective than isotretinoin** for severe, nodulocystic acne or acne with sinus tracts and is not a definitive cure. *Doxycycline* - Doxycycline is another **oral tetracycline antibiotic** commonly used for moderate to severe inflammatory acne due to its anti-inflammatory effects and reduction of *C. acnes*. - Similar to minocycline, it is a good option for inflammatory acne but **insufficient for very severe, recalcitrant acne** with sinus tracts, where isotretinoin is superior. *Topical dapsone* - Topical dapsone is an **anti-inflammatory agent** primarily used for mild to moderate inflammatory acne, particularly papules and pustules. - It is **not effective for severe nodulocystic acne** or acne associated with sinus tracts and would not be appropriate as monotherapy for this presentation.
Question 10: A patient presents with skin lesions and erosions on the buccal mucosa. The immunofluorescence image is shown. What is the most likely diagnosis?
- A. Bullous pemphigoid
- B. Pemphigus vulgaris (Correct Answer)
- C. Linear IgA disease
- D. Dermatitis herpetiformis
Explanation: ***Pemphigus vulgaris*** - The combination of **flaccid blisters/erosions** on the skin and **buccal mucosal lesions** is characteristic of pemphigus vulgaris. The image showing **intercellular IgG deposits** (a "chicken wire" pattern) in the epidermis confirms the diagnosis on immunofluorescence. - Pemphigus vulgaris is an **autoimmune blistering disease** caused by autoantibodies against **desmoglein 1 and 3**, leading to acantholysis (loss of cell adhesion) within the epidermis. *Bullous pemphigoid* - This condition typically presents with **tense bullae** that are less prone to rupture, and **mucosal involvement is rare**. - Immunofluorescence in bullous pemphigoid shows **linear IgG and C3 deposits at the dermoepidermal junction**, not an intercellular epidermal pattern. *Linear IgA disease* - Characterized by **linear IgA deposition along the basement membrane zone** on direct immunofluorescence. - Clinically, it presents with **blisters** that can be variable in appearance, but the pathognomonic immunofluorescence pattern is distinct. *Dermatitis herpetiformis* - Presents with very **pruritic vesicles and papules**, primarily on extensor surfaces, and is strongly associated with **celiac disease**. - Direct immunofluorescence reveals **granular IgA deposits in the dermal papillae**, which is distinct from the intercellular IgG pattern seen here.