All SubjectsAnatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q11
Which artery is palpated behind the medial malleolus and in front of the Achilles tendon?
Q12
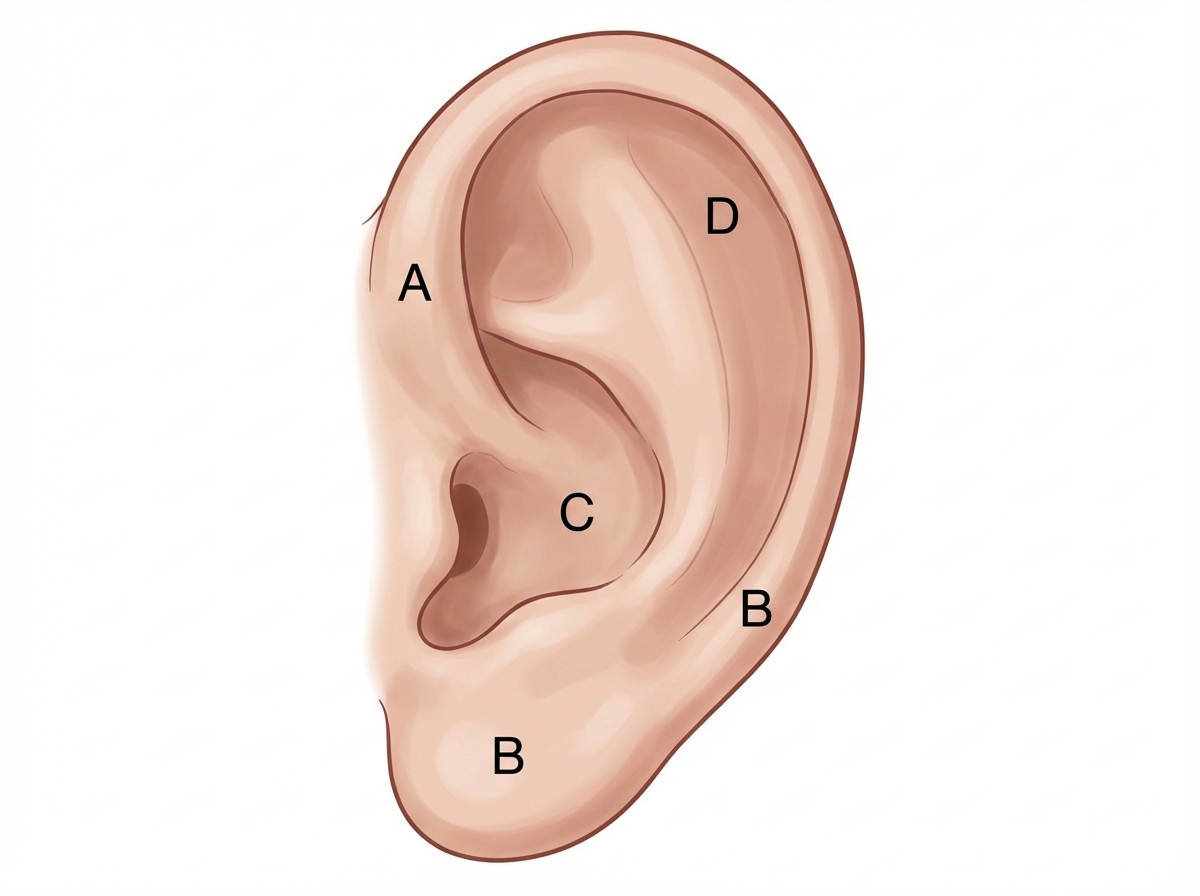
Match the following nerves to their respective areas of supply to the auricle
Q13
A patient diagnosed with sciatica has tender hamstrings. Which of the following nerves supplies a hybrid muscle that is partially spared in this patient?
Q14
What is the most common site of congenital diaphragmatic hernia?
Q15
A patient with a nerve injury was asked to form an "O" with their index finger and thumb but was unable to do so. Which muscle is most likely affected?
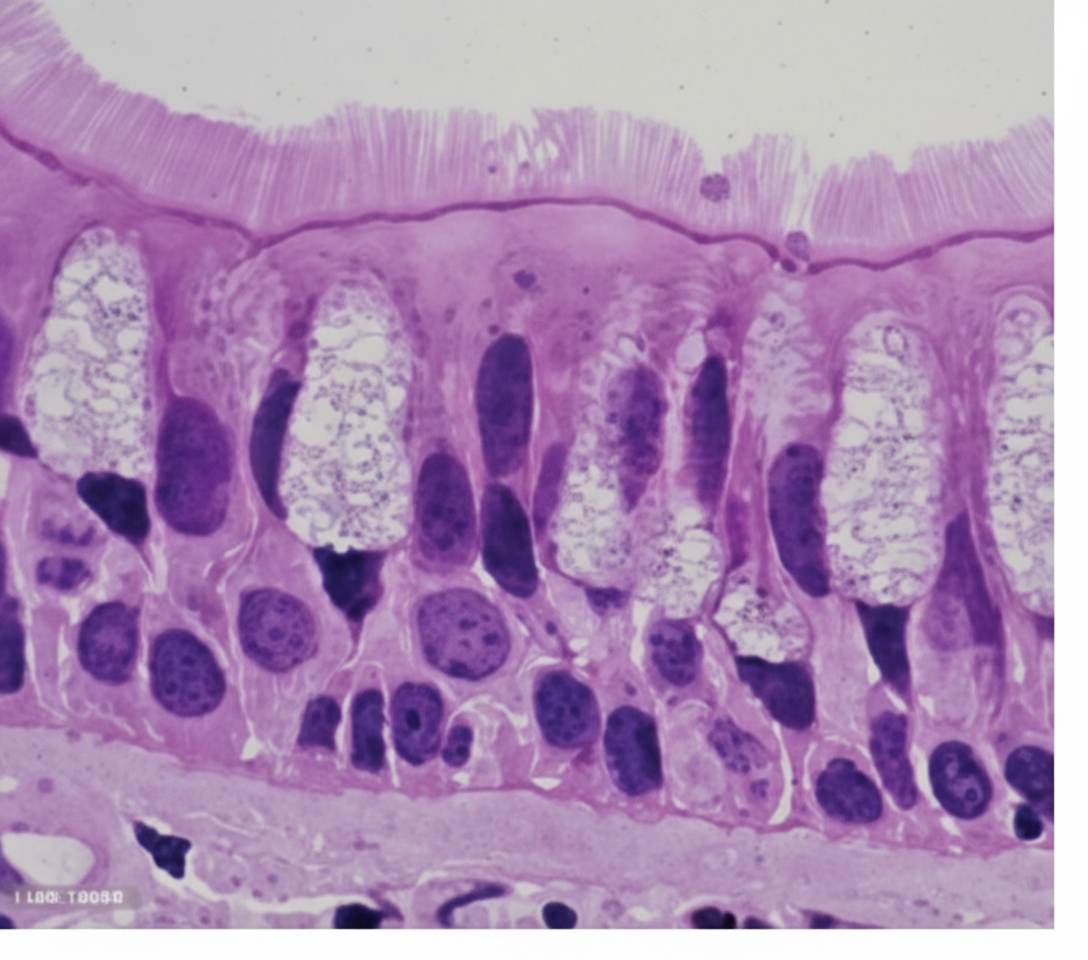
Q16
This type of epithelium is most commonly seen in which of the following organs?
Q17
Which tongue papillae do not have taste buds?
Q18
Impaired gag reflex is seen due to a lesion in which cranial nerves?
Q19
A slipped disc at the level shown in the image would most likely involve which nerve root?

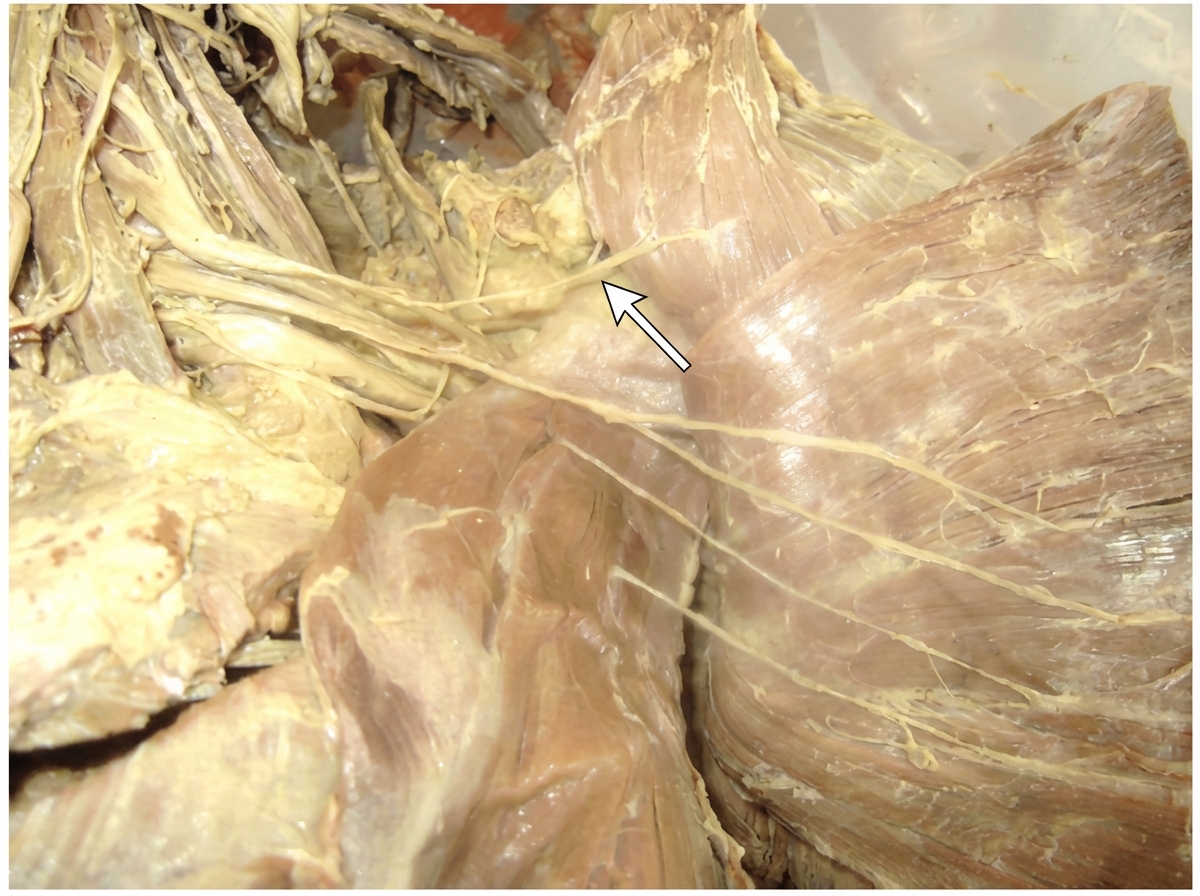
Q20
Identify the arrow marked nerve