NEET-PG 2024 — Anatomy
23 Previous Year Questions with Answers & Explanations
At what age does maximum brain growth occur?
The Image shows the growth curve of different organs with age. Identify A in the graph
Identify the uterus shown in the image?
Linear growth of bone is disturbed when a fracture occurs in which part?
The "O sign" formed by the thumb and index finger is affected. Which muscle is most likely injured?
An absent gag reflex can result from injury to which of the following nerves?
Identify the arrow marked nerve 
Identify the labeling correctly 
The nerve passing through the arrow-marked region in the provided image has been lesioned. Which of the following is the most likely clinical presentation?
The covering of an omphalocele is derived from which of the following layers?
NEET-PG 2024 - Anatomy NEET-PG Practice Questions and MCQs
Question 1: At what age does maximum brain growth occur?
- A. 6 months (Correct Answer)
- B. 1 year
- C. 2 years
- D. 3 years
- E. 5 years
Explanation: ***6 months*** - **Brain growth** is most rapid during the early postnatal period, with the brain reaching almost **50% of its adult size by 6 months of age**. - This period involves rapid **synaptogenesis** and myelination, crucial for early cognitive and motor development. *1 year* - While significant **brain growth** continues, the peak rate of increase in brain volume has typically passed by 1 year. - At this age, the brain has reached approximately **75% of its adult size**. *2 years* - By 2 years, the brain is about **80% of its adult size**, indicating ongoing but slower growth compared to the first year. - This period is more characterized by refinement of neural circuits rather than rapid volumetric expansion. *3 years* - At 3 years, the brain has attained around **90% of its adult size**, though important developmental changes continue. - The rate of **neural development** at this stage largely focuses on strengthening existing connections and pruning less used ones. *5 years* - By 5 years, the brain has reached approximately **90-95% of its adult size**, with growth significantly slower than in earlier years. - Development at this age focuses primarily on **synaptic pruning** and refinement of neural networks rather than volumetric growth.
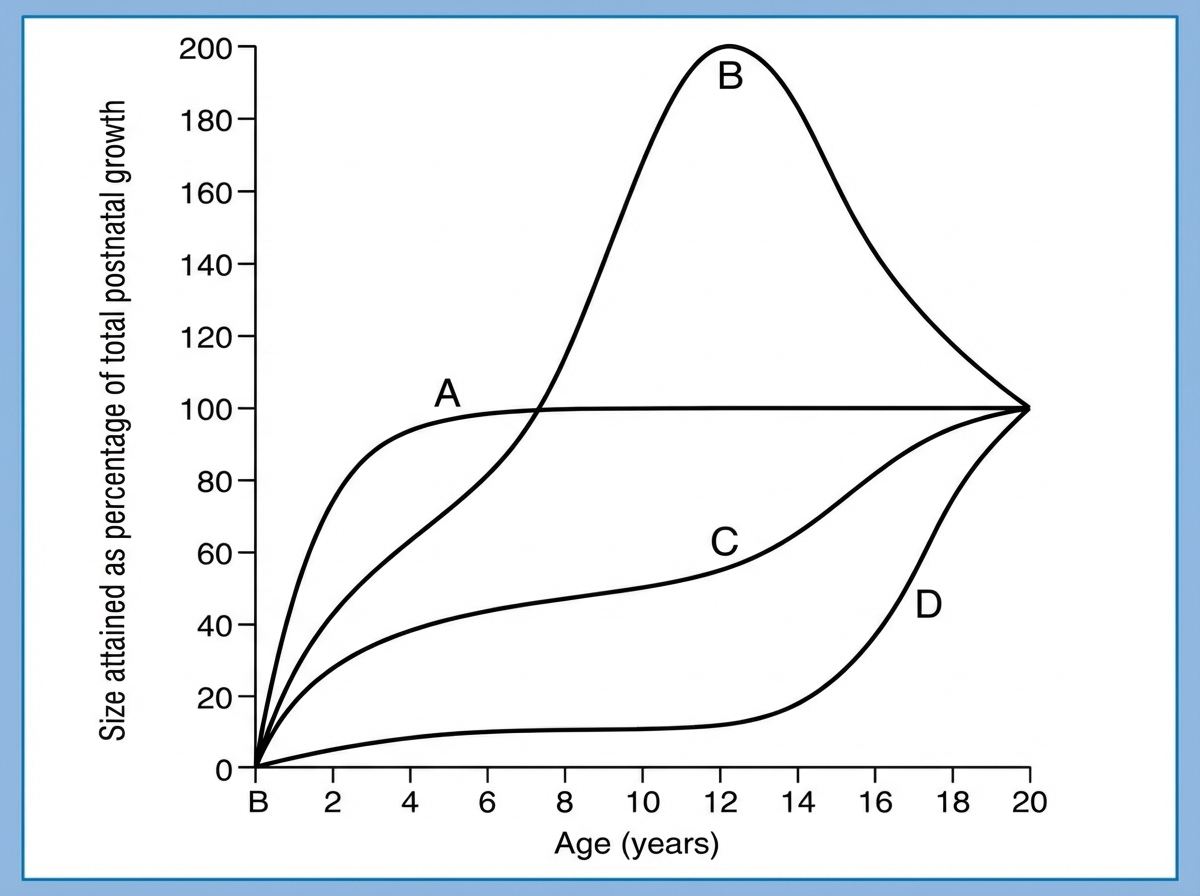
Question 2: The Image shows the growth curve of different organs with age. Identify A in the graph
- A. Brain Growth (Correct Answer)
- B. Somatic Growth
- C. Lymphoid Growth
- D. Gonadal Growth
- E. Reproductive Growth
Explanation: ***Brain Growth*** - This graph shows a rapid increase in size during early childhood, reaching near-adult proportions by age 5-6, which is characteristic of **brain development**. - The brain undergoes significant myelinization and neuronal growth in the first few years of life, reflected in this steep curve. *Somatic Growth* - **Somatic growth** (body as a whole) generally follows a more gradual S-shaped curve, with two major growth spurts: one in infancy and another during puberty. - It does not plateau as early as curve A, but continues to increase significantly through adolescence. *Lymphoid Growth* - **Lymphoid tissues** (e.g., thymus, lymph nodes) show a unique growth pattern, peaking in size around 10-12 years of age and then involuting or decreasing in size during adolescence. - This pattern is distinctly different from curve A, which continuously increases and plateaus. *Gonadal Growth* - **Gonadal growth** (reproductive organs) typically shows minimal growth during childhood, with a pronounced and rapid increase in size starting at puberty (around 10-14 years of age). - This growth pattern is a later and more delayed surge compared to what is depicted in curve A. *Reproductive Growth* - **Reproductive growth** follows essentially the same pattern as gonadal growth, with minimal development during childhood and rapid acceleration during puberty. - Like gonadal tissues, reproductive organs show their major growth spurt much later than the early plateau seen in curve A.
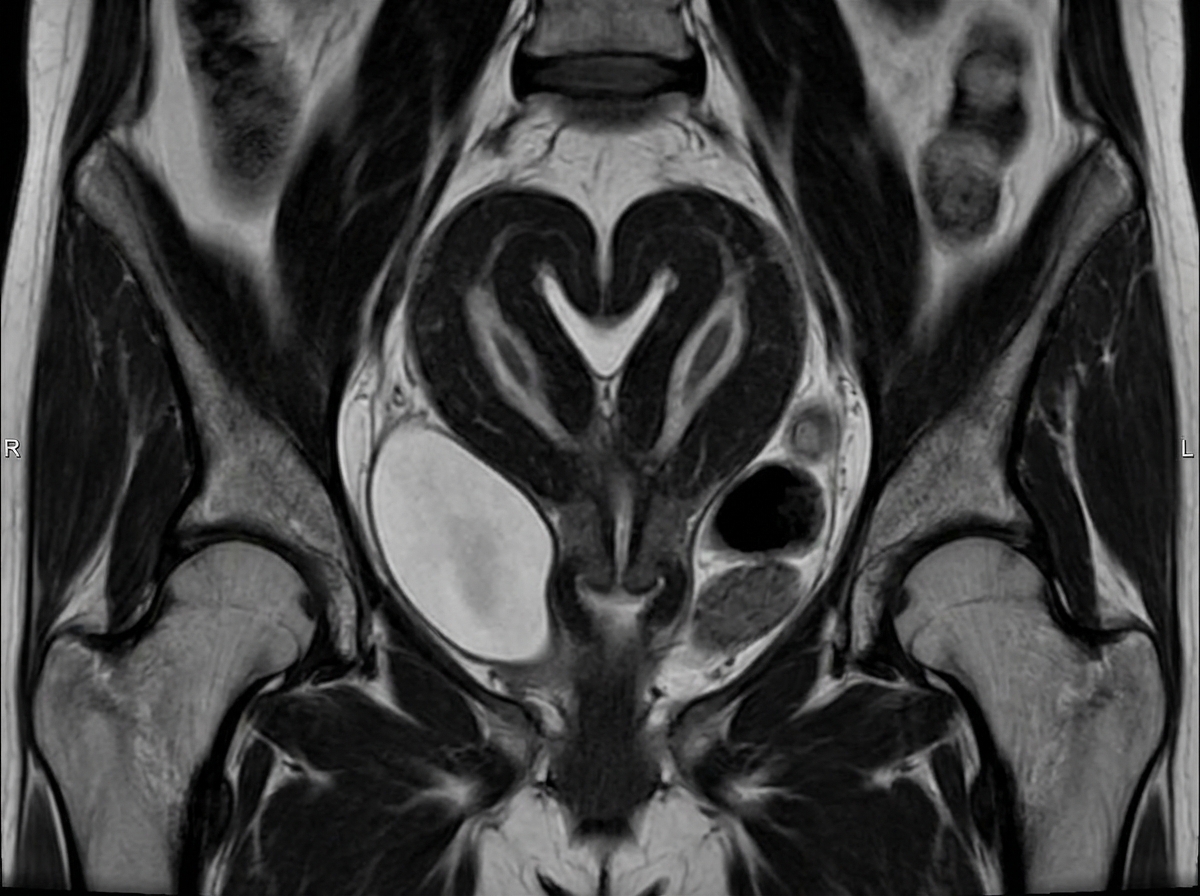
Question 3: Identify the uterus shown in the image?
- A. Bicornuate (Correct Answer)
- B. Didelphys
- C. Arcuate
- D. Septate
- E. Unicornuate
Explanation: ***Bicornuate*** - The image displays a uterus with two distinct uterine horns that are partially fused at the fundus, creating a **heart-shaped external indentation**. - This morphology is characteristic of a **bicornuate uterus**, which results from incomplete fusion of the paramesonephric (Müllerian) ducts. *Didelphys* - A **uterus didelphys** would show two completely separate uteri, each with its own cervix and often a separate vagina. - The image clearly shows a single cervix and a single vaginal canal, with only the upper uterine body being divided. *Arcuate* - An **arcuate uterus** has a small, concave indentation at the fundus, but the overall shape is typically that of a normal uterus with a mild deformity. - The image shows a much more significant division of the uterine cavity than seen in an arcuate uterus. *Septate* - A **septate uterus** has a normal external contour but contains an internal septum that divides the uterine cavity into two parts. - The image demonstrates both internal and external division with a heart-shaped fundal indentation, which distinguishes bicornuate from septate uterus. *Unicornuate* - A **unicornuate uterus** results from failure of one Müllerian duct to develop, creating a single elongated uterine horn. - The image shows two uterine horns, not a single horn, ruling out this diagnosis.
Question 4: Linear growth of bone is disturbed when a fracture occurs in which part?
- A. Epiphysis
- B. Diaphysis
- C. Metaphysis
- D. Epiphyseal plate (Correct Answer)
- E. Periosteum
Explanation: ***Epiphyseal plate*** - The **epiphyseal plate**, also known as the **growth plate**, is a cartilaginous disc responsible for the **longitudinal growth** of long bones. - A fracture in this region can damage the **chondrocytes** and disrupt the normal process of endochondral ossification, leading to **growth arrest** or limb length discrepancy. *Epiphysis* - The **epiphysis** is the end part of a long bone, often covered by **articular cartilage**, forming a joint. - While an epiphyseal fracture can affect joint function, it typically does not directly disturb the **linear growth** of the bone unless it extends into the growth plate. *Diaphysis* - The **diaphysis** is the main or midsection of a long bone, composed primarily of **compact bone**. - Fractures in the diaphysis generally heal through **callus formation** and remodeling, usually without significantly impacting the overall **linear growth** of the bone. *Metaphysis* - The **metaphysis** is the wider portion of a long bone, adjacent to the growth plate and diaphysis. - Though highly vascular, fractures to the metaphysis usually heal well and do not directly control **linear bone growth** like the epiphyseal plate. *Periosteum* - The **periosteum** is the fibrous membrane covering the outer surface of bones, important for **appositional growth** (bone widening) and fracture healing. - While it contains osteogenic cells that contribute to bone repair and thickness, it does not control **longitudinal bone growth**, which is the function of the epiphyseal plate.
Question 5: The "O sign" formed by the thumb and index finger is affected. Which muscle is most likely injured?
- A. Opponens pollicis
- B. Flexor pollicis longus (Correct Answer)
- C. Flexor pollicis brevis
- D. Abductor pollicis brevis
- E. Flexor digitorum profundus (index finger)
Explanation: ***Flexor pollicis longus*** - The **"O sign"** (or **"OK sign"**) tests the ability to form a tight **tip-to-tip pinch** between the thumb and index finger, creating a circular "O" shape. - This requires **flexion of the thumb interphalangeal (IP) joint** via the **flexor pollicis longus (FPL)** and **flexion of the index finger distal interphalangeal (DIP) joint** via the **flexor digitorum profundus (FDP)**. - Both FPL and FDP to the index/middle fingers are innervated by the **anterior interosseous nerve (AIN)**, a branch of the median nerve. - **AIN palsy** results in inability to flex the thumb IP and index DIP joints, causing the **"O sign"** to become flattened (pinch sign or **"teardrop sign"**). - Injury to **FPL** specifically impairs thumb IP flexion, directly affecting the ability to form the **"O sign"**. *Flexor digitorum profundus (index finger)* - The **FDP to the index finger** is also innervated by the **AIN** and is essential for flexing the DIP joint of the index finger. - Isolated FDP injury would affect the index finger's contribution to the "O sign" but both FPL and FDP are typically affected together in AIN palsy. - This is a plausible answer, making this a higher-order question testing understanding of the anatomy. *Opponens pollicis* - The **opponens pollicis** enables **opposition** of the thumb, bringing the thumb pad to the finger pads (pad-to-pad pinch). - It is innervated by the **recurrent branch of the median nerve**, not the AIN. - Opposition is different from the **tip-to-tip pinch** required for the "O sign," which requires IP joint flexion, not just opposition at the carpometacarpal joint. *Flexor pollicis brevis* - The **flexor pollicis brevis** flexes the thumb at the **metacarpophalangeal (MCP) joint**, not the IP joint. - The superficial head is innervated by the recurrent branch of the median nerve, while the deep head is innervated by the ulnar nerve. - While it contributes to thumb flexion, it does not flex the thumb IP joint, which is essential for forming the **"O sign"**. *Abductor pollicis brevis* - The **abductor pollicis brevis** abducts the thumb away from the palm in a plane perpendicular to the palm. - It is innervated by the **recurrent branch of the median nerve**. - Abduction is not required for forming the **"O sign"**, which primarily tests flexion at the IP and DIP joints.
Question 6: An absent gag reflex can result from injury to which of the following nerves?
- A. Cranial Nerve VII (Facial) and Cranial Nerve V (Trigeminal)
- B. Cranial Nerve V (Trigeminal) and Cranial Nerve IX (Glossopharyngeal)
- C. Cranial Nerve IX (Glossopharyngeal) and Cranial Nerve X (Vagus) (Correct Answer)
- D. Cranial Nerve X (Vagus) and Cranial Nerve VII (Facial)
- E. Cranial Nerve XII (Hypoglossal) and Cranial Nerve X (Vagus)
Explanation: ***Cranial Nerve IX (Glossopharyngeal) and Cranial Nerve X (Vagus)*** - The **gag reflex** is a protective reflex that involves both sensory and motor components. - The **glossopharyngeal nerve (CN IX)** is responsible for the **afferent (sensory)** limb, detecting stimulation of the posterior pharynx. The **vagus nerve (CN X)** is responsible for the **efferent (motor)** limb, causing contraction of pharyngeal muscles. *Cranial Nerve VII (Facial) and Cranial Nerve V (Trigeminal)* - The **facial nerve (CN VII)** primarily controls muscles of **facial expression** and taste from the anterior two-thirds of the tongue. - The **trigeminal nerve (CN V)** mediates sensation to the face, mastication, and corneal reflex, but not the gag reflex. *Cranial Nerve V (Trigeminal) and Cranial Nerve IX (Glossopharyngeal)* - While **CN IX** is indeed involved in the **sensory component of the gag reflex**, the **trigeminal nerve (CN V)** is not directly involved in either the sensory or motor pathway of the gag reflex. - The trigeminal nerve's primary roles are facial sensation and mastication. *Cranial Nerve X (Vagus) and Cranial Nerve VII (Facial)* - The **vagus nerve (CN X)** is crucial for the **motor component** of the gag reflex. - However, the **facial nerve (CN VII)** is not involved in the gag reflex; its functions relate to facial movement and taste. *Cranial Nerve XII (Hypoglossal) and Cranial Nerve X (Vagus)* - While the **vagus nerve (CN X)** does provide the **motor component** of the gag reflex, the **hypoglossal nerve (CN XII)** is not involved in this reflex. - The **hypoglossal nerve (CN XII)** controls intrinsic and extrinsic muscles of the tongue, important for tongue movement and speech, but not for the pharyngeal muscle contraction required for the gag reflex.
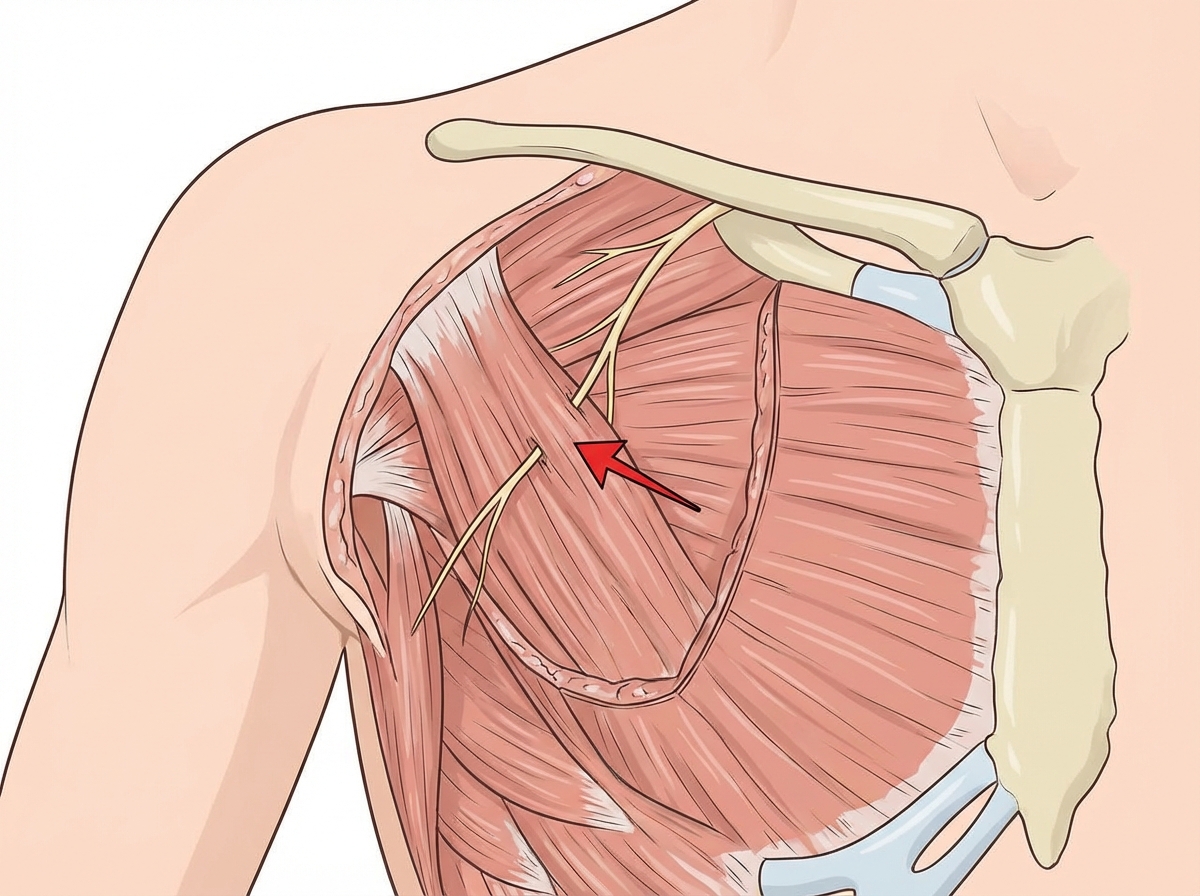
Question 7: Identify the arrow marked nerve 
- A. Long thoracic nerve
- B. Thoracodorsal nerve
- C. Lateral pectoral nerve
- D. Medial pectoral nerve (Correct Answer)
- E. Suprascapular nerve
Explanation: ***Medial pectoral nerve*** - The arrow points to a nerve that is seen perforating the **pectoralis minor muscle**. This is a key anatomical landmark for the **medial pectoral nerve**. - This nerve supplies both the **pectoralis major** and **pectoralis minor** muscles, originating from the medial cord of the brachial plexus. *Long thoracic nerve* - The **long thoracic nerve** typically runs superficial to the serratus anterior muscle, not perforating the pectoralis minor. - Injury to this nerve results in **winged scapula** due to paralysis of the serratus anterior, which is distinct from the function of the nerve shown. *Thoracodorsal nerve* - The **thoracodorsal nerve** primarily innervates the **latissimus dorsi muscle** and typically runs along the lateral border of the scapula and axilla, not in the anterior chest wall where the pectoralis minor is located. - It arises from the **posterior cord of the brachial plexus**. *Lateral pectoral nerve* - The **lateral pectoral nerve** arises from the lateral cord and typically supplies only the **pectoralis major muscle**. - It often passes **medial to the pectoralis minor muscle** or penetrates the muscle from a more lateral aspect, but does not perforate it in the characteristic way shown for the medial pectoral nerve. *Suprascapular nerve* - The **suprascapular nerve** arises from the **upper trunk of the brachial plexus** and passes through the **suprascapular notch** beneath the superior transverse scapular ligament. - It innervates the **supraspinatus** and **infraspinatus** muscles and is located in the posterior shoulder region, not in the anterior chest wall where the structure shown is located.
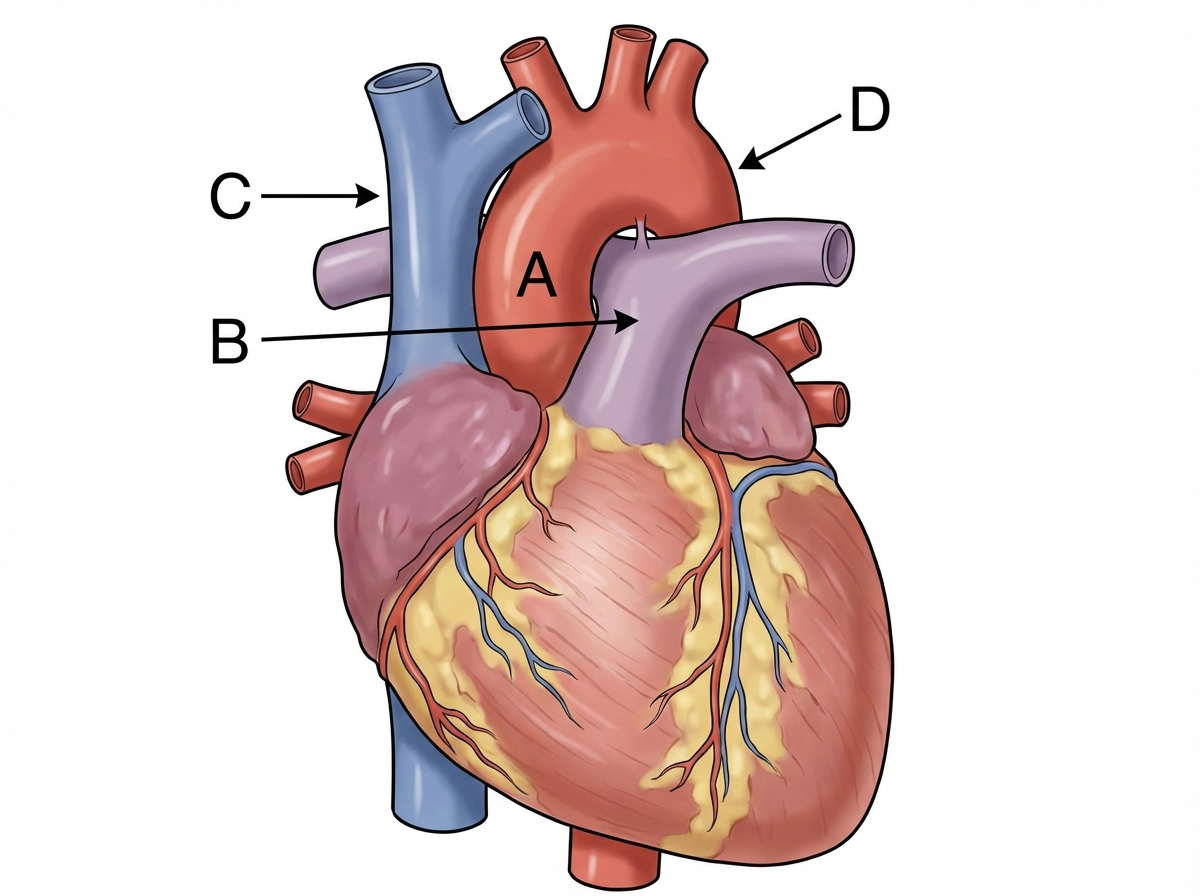
Question 8: Identify the labeling correctly 
- A. A - Ascending aorta, B - Pulmonary trunk, C - Superior vena cava, D - Descending aorta (Correct Answer)
- B. A - Ascending aorta, B - Superior vena cava, C - Pulmonary trunk, D - Descending aorta
- C. A - Superior vena cava, B - Pulmonary trunk, C - Ascending aorta, D - Descending aorta
- D. A - Pulmonary trunk, B - Ascending aorta, C - Superior vena cava, D - Descending aorta
- E. A - Ascending aorta, B - Pulmonary trunk, C - Descending aorta, D - Superior vena cava
Explanation: ***A - Ascending aorta, B - Pulmonary trunk, C - Superior vena cava, D - Descending aorta*** - **A** points to the **ascending aorta**, the initial segment of the aorta emerging from the left ventricle. - **B** indicates the **pulmonary trunk**, which originates from the right ventricle and carries deoxygenated blood to the lungs. - **C** correctly identifies the **superior vena cava**, responsible for draining deoxygenated blood from the upper body into the right atrium. - **D** is correctly labeled as the **descending aorta**, the portion of the aorta that descends through the thorax and abdomen. *A - Ascending aorta, B - Superior vena cava, C - Pulmonary trunk, D - Descending aorta* - This option incorrectly identifies **B as superior vena cava** and **C as pulmonary trunk**. B is clearly emerging from the right ventricle, characteristic of the pulmonary trunk, while C is positioned where the superior vena cava would be. - The superior vena cava (C) would be located to the right and anterior to the ascending aorta, while the pulmonary trunk (B) is anterior to the ascending aorta, emerging from the right ventricle. *A - Superior vena cava, B - Pulmonary trunk, C - Ascending aorta, D - Descending aorta* - This option incorrectly labels **A as superior vena cava** and **C as ascending aorta**. A is clearly the large vessel emerging from the left side of the heart, consistent with the ascending aorta. - The ascending aorta (A) would be the largest vessel emerging from the left ventricle, and the superior vena cava (C) would be entering the right atrium. *A - Pulmonary trunk, B - Ascending aorta, C - Superior vena cava, D - Descending aorta* - This option incorrectly identifies **A as pulmonary trunk** and **B as ascending aorta**. A is the large vessel originating from the left ventricle, which is the ascending aorta. - The pulmonary trunk (B) arises from the right ventricle and is usually anterior to the ascending aorta (A). *A - Ascending aorta, B - Pulmonary trunk, C - Descending aorta, D - Superior vena cava* - This option incorrectly swaps **C and D**, labeling C as descending aorta and D as superior vena cava. C is positioned in the superior mediastinum where the superior vena cava enters the right atrium, not in the posterior mediastinum where the descending aorta would be located. - The descending aorta (D) runs posteriorly in the thorax, while the superior vena cava (C) is an anterior structure draining into the right atrium.
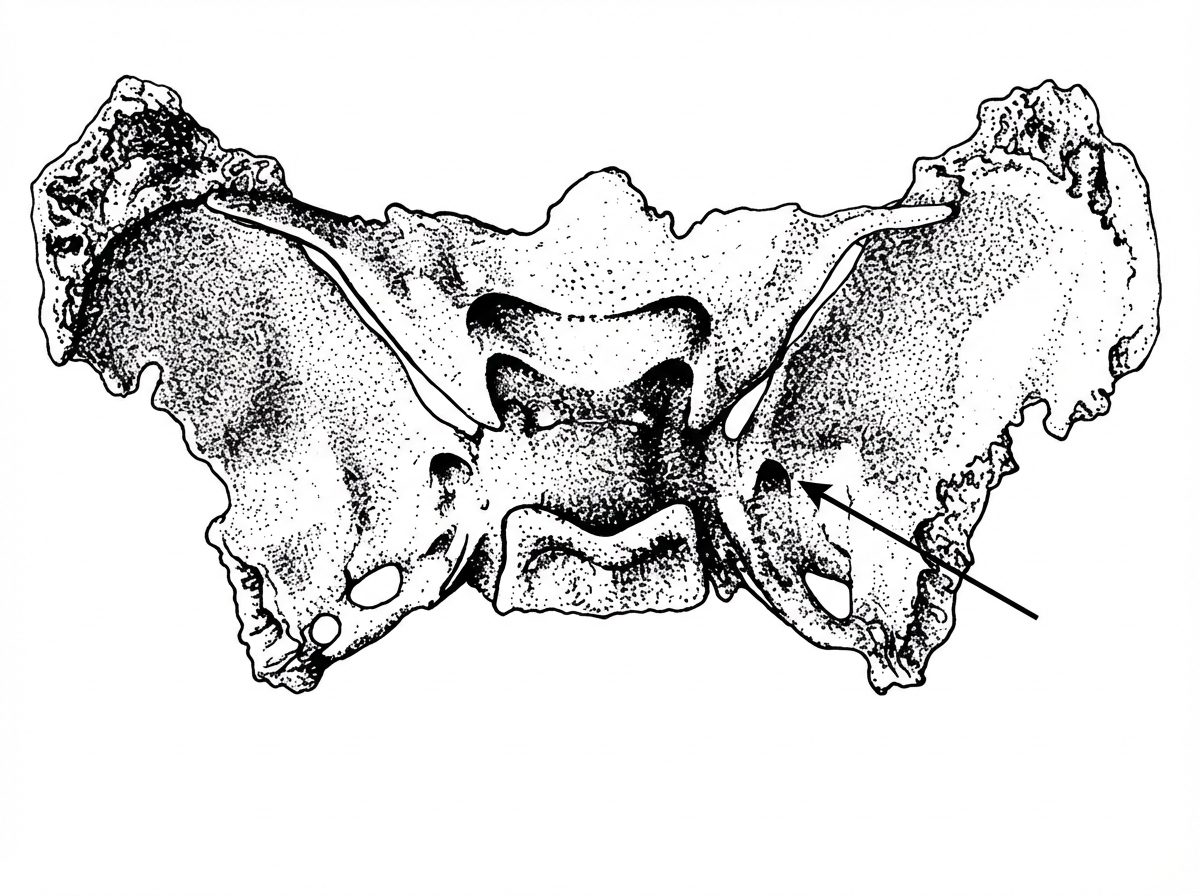
Question 9: The nerve passing through the arrow-marked region in the provided image has been lesioned. Which of the following is the most likely clinical presentation?
- A. Loss of sensation in the jaw area
- B. Loss of sensation on the scalp and nose
- C. Loss of sensation in the maxillary area of the face (Correct Answer)
- D. Loss of sensation in the mucosa of nasopharynx
- E. Loss of motor function to muscles of facial expression
Explanation: ***Loss of sensation in the maxillary area of the face*** - The arrow points to the **foramen rotundum**, which transmits the **maxillary nerve (V2)**, a branch of the trigeminal nerve. - Lesion of the maxillary nerve (V2) leads to sensory loss in the **maxillary region of the face**, including the cheek, upper lip, upper teeth, and palate. *Loss of sensation in the jaw area* - Sensation in the jaw area, including the lower teeth and chin, is primarily supplied by the **mandibular nerve (V3)**, which exits through the foramen ovale. - A lesion at the foramen rotundum would not directly affect V3. *Loss of sensation on the scalp and nose* - Sensation to the scalp (anterior part) and nose is primarily supplied by the **ophthalmic nerve (V1)**, which exits the skull through the superior orbital fissure. - The foramen rotundum is not involved in the passage of the ophthalmic nerve. *Loss of sensation in the mucosa of nasopharynx* - While parts of the nasopharynx mucosa receive innervation from V2, this is a very specific and limited area, and the primary and most prominent sensory loss from a V2 lesion would be in the **maxillary facial region**. - Other nerves like the glossopharyngeal nerve also contribute to nasopharyngeal sensation. *Loss of motor function to muscles of facial expression* - Motor function to muscles of facial expression is supplied by the **facial nerve (CN VII)**, not the maxillary nerve (V2). - The maxillary nerve is a purely **sensory** branch of the trigeminal nerve and has no motor function. - The facial nerve exits the skull through the stylomastoid foramen, not the foramen rotundum.
Question 10: The covering of an omphalocele is derived from which of the following layers?
- A. Amnion (Correct Answer)
- B. Chorion
- C. Mesoderm
- D. Endoderm
- E. Ectoderm
Explanation: ***Amnion*** - An **omphalocele** is a congenital abdominal wall defect where abdominal contents protrude through the umbilical ring, covered by a sac derived from the **amnion** and peritoneum. - The covering of an omphalocele defect is an intact peritoneal sac that is covered externally by **amnion**. *Chorion* - The **chorion** is the outermost membrane surrounding an embryo, providing protection and nourishment, but it does not form the covering of an omphalocele. - It works in conjunction with the decidua to form the **placenta** and has finger-like projections called villi on its outer surface. *Mesoderm* - The **mesoderm** is one of the three primary germ layers in embryonic development, giving rise to connective tissue, muscle, and blood cells. - **Fetal skin**, not the omphalocele covering, develops from the mesoderm and ectoderm. *Endoderm* - The **endoderm** is the innermost of the three primary germ layers, giving rise to the lining of the digestive tract and respiratory system. - The omphalocele covering is derived from the amnion, not the endoderm, which is involved in forming internal organs. *Ectoderm* - The **ectoderm** is the outermost of the three primary germ layers, giving rise to the nervous system, skin epidermis, and sensory organs. - While ectoderm contributes to skin development, the omphalocele sac is specifically covered by amnion, not ectodermal derivatives.