NEET-PG 2022 — Surgery
8 Previous Year Questions with Answers & Explanations
Which of the following is a primary aim of damage control laparotomy?
What type of wound is characterized by the scraping away of the skin?
What is the preferred method for removing a foreign body from the lung in children?
An elderly male patient presented with a sudden onset of scrotal pain and discharge as shown in the image. What is the likely diagnosis?

The image below shows a pressure sore. Which stage does this belong to?

Identify the most common site of an intraperitoneal abscess.
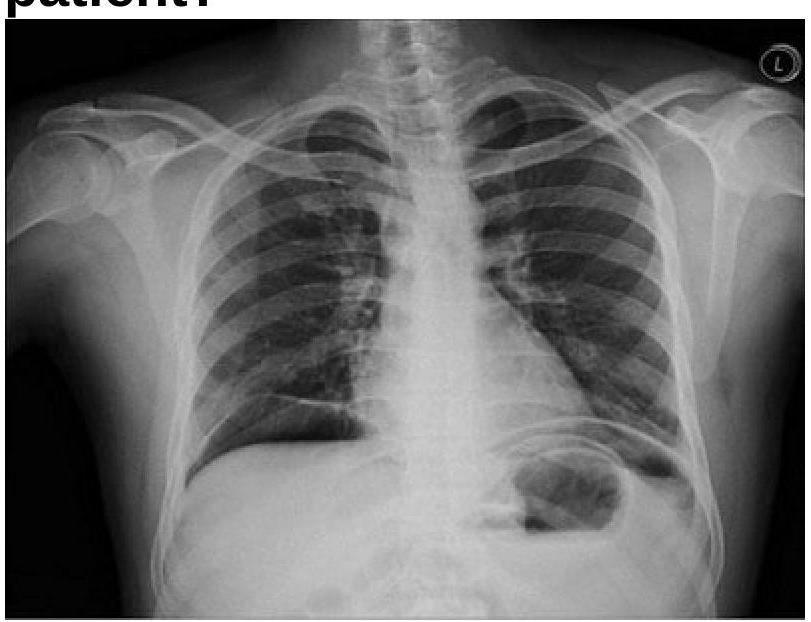
A 40 years old male was brought emergency with severe abdominal pain. On examination, pulse rate was 112/minute and systolic BP was 80 mmHg. Chest x-ray is given below. What is the most appropriate management?
While shaving, a 45-year-old teacher notices a marble-sized mass beneath his left ear. The mass is eventually excised, revealing which of the following benign parotid gland lesions?
NEET-PG 2022 - Surgery NEET-PG Practice Questions and MCQs
Question 1: Which of the following is a primary aim of damage control laparotomy?
- A. Arrest hemorrhage and control contamination. (Correct Answer)
- B. Control contamination
- C. Prevent coagulopathy
- D. Arrest hemorrhage
Explanation: ***Arrest hemorrhage and control contamination.*** * The overarching goal of a **damage control laparotomy** is to rapidly address immediate life threats, primarily **hemorrhage** and **bowel contamination**, in severely injured, unstable patients. * This approach prioritizes patient survival by performing essential steps quickly, deferring definitive repairs until the patient is physiologically stable. *Control contamination* * While **controlling contamination** is a critical component of damage control laparotomy, it is not the sole primary aim. * Uncontrolled bleeding, even without contamination, can rapidly lead to death in a trauma patient. *Prevent coagulopathy* * Preventing **coagulopathy** is an important consideration during damage control, but it is a consequence of uncontrolled hemorrhage and hypothermia, rather than a primary surgical aim in the initial damage control phase. * The surgical steps in damage control directly address the sources of bleeding and contamination. *Arrest hemorrhage* * **Arresting hemorrhage** is indeed a primary aim, but it is often accompanied by the need to control contamination from injured hollow organs. * Many abdominal trauma cases involve both significant bleeding and potential contamination.
Question 2: What type of wound is characterized by the scraping away of the skin?
- A. Superficial wound
- B. Tear in the skin
- C. Abrasion (Correct Answer)
- D. Deep tissue injury
Explanation: ***Abrasion*** - An **abrasion** is a wound caused by the **scraping or rubbing away of the superficial layers of the skin** (epidermis and sometimes superficial dermis). - It typically results from a fall or friction against a rough surface, common in children's scraped knees or elbows. *Superficial wound* - This is a **general term** and does not specifically describe the mechanism of injury as scraping. - A superficial wound could be a **minor cut or scratch** that doesn't involve scraping. *Tear in the skin* - A **tear in the skin** refers to a **laceration**, which is a wound caused by tearing of soft body tissue, often resulting in irregular edges. - This is distinct from the scraping action characteristic of an abrasion, where tissue is rubbed away rather than torn. *Deep tissue injury* - A **deep tissue injury (DTI)** is a **pressure-related injury** characterized by intact skin with **discoloration** (e.g., maroon or purple) or a blood-filled blister due to damage of underlying soft tissue. - It is not caused by external scraping and involves deeper tissue layers affected by prolonged pressure.
Question 3: What is the preferred method for removing a foreign body from the lung in children?
- A. Rigid bronchoscopy (Correct Answer)
- B. Chest x-ray
- C. Flexible endoscopy
- D. Direct laryngoscopy
Explanation: ***Rigid bronchoscopy*** - **Rigid bronchoscopy** is the preferred method for removing foreign bodies from the lung in children due to its ability to provide better air control, magnified viewing, and larger working channels for robust grasping tools. - It allows for complete ventilation control and isolation of the airway, which is crucial in children where airway obstruction can rapidly lead to respiratory compromise. *Chest x-ray* - A **chest x-ray** is a diagnostic tool used to identify the presence and location of a foreign body, but it is not a method for removal. - Many foreign bodies, especially non-radiopaque ones like food, may not be visible on an x-ray, making it unreliable for definitive diagnosis of presence or absence. *Flexible endoscopy* - While **flexible bronchoscopy** can be used for foreign body removal in some adults or specific situations, it is generally less effective and carries higher risks in children, especially for larger or lodged objects. - Its smaller working channels and less stable airway control make it less suitable for urgent and complete removal in the pediatric population. *Direct laryngoscopy* - **Direct laryngoscopy** is used to visualize the larynx and vocal cords, primarily to remove foreign bodies from the upper airway or intubate, but not typically for removal of foreign bodies lodged deep within the main bronchi or lungs. - It does not offer direct access or visualization of the lower bronchial tree where most aspirated foreign bodies in children tend to lodge.
Question 4: An elderly male patient presented with a sudden onset of scrotal pain and discharge as shown in the image. What is the likely diagnosis?
- A. Fournier’s gangrene (Correct Answer)
- B. Torsion of testis
- C. Scrotal carcinoma
- D. Acute epididymo-orchitis
Explanation: ***Fournier's gangrene*** - The sudden onset of scrotal pain with discharge in an elderly male, combined with **tissue necrosis** and extensive scrotal skin changes, is characteristic of **Fournier's gangrene** (necrotizing fasciitis of the genitalia). - Elderly males are at higher risk due to **diabetes**, **immunocompromise**, and **urogenital infections**, making this a rapidly progressive and potentially life-threatening condition requiring urgent surgical debridement. *Acute epididymo-orchitis* - While epididymo-orchitis can cause scrotal pain and discharge, it typically does **not cause tissue necrosis** or the extensive scrotal skin changes described. - It presents as **localized inflammation** of the epididymis/testis without the widespread necrotizing changes seen in this case. *Torsion of testis* - Testicular torsion typically presents with **abrupt, severe scrotal pain** and swelling, but usually **without discharge** or the extensive scrotal skin changes seen here. - It constitutes a **surgical emergency** due to compromised blood supply to the testis, but doesn't involve necrotizing infection. *Scrotal carcinoma* - Scrotal carcinoma usually presents as a **painless mass or ulceration** that grows over time, rather than a sudden onset of severe pain and discharge. - It represents a **chronic process** and doesn't typically cause the acute necrotizing inflammatory changes observed in this case.
Question 5: The image below shows a pressure sore. Which stage does this belong to?
- A. Stage 1
- B. Stage 2
- C. Stage 3
- D. Stage 4 (Correct Answer)
Explanation: ***Stage 4*** - The image clearly shows **extensive tissue loss**, including exposed bone and muscle, indicating a **deep tissue injury**. - The presence of large areas of **dead tissue (eschar)**, undermining, and tunneling are characteristic features of a stage 4 pressure sore. *Stage 1* - This stage involves **intact skin** with non-blanchable redness, indicating only superficial damage. - There is no **break in the skin** or tissue loss in Stage 1 pressure sores. *Stage 2* - Characterized by **partial-thickness skin loss**, presenting as an open blister or shallow ulcer. - **No visible deeper tissue** such as fat, muscle, or bone is exposed in this stage. *Stage 3* - Involves **full-thickness skin loss** with visible subcutaneous fat, but bone, tendon, or muscle are not exposed. - While there may be **undermining or tunneling**, the deep structures are not yet visible as seen in the image.
Question 6: Identify the most common site of an intraperitoneal abscess.
- A. Suprahepatic
- B. Left subphrenic space
- C. Pelvis (Pouch of Douglas) (Correct Answer)
- D. Subhepatic
Explanation: ***Pelvis (Pouch of Douglas)*** - The **Pouch of Douglas** (rectouterine or rectovesical pouch) is the **most common site** for intraperitoneal abscesses. - It is the **most dependent (lowest) part** of the peritoneal cavity in both upright and supine positions, allowing gravity to facilitate collection of infected fluid. - Commonly results from **perforated appendicitis**, **diverticulitis**, **gynecological infections** (PID, tubo-ovarian abscess), or any source of peritoneal contamination where infected material flows downward. - **Clinical significance**: Pelvic abscesses can be drained via transrectal or transvaginal approaches, making them accessible for percutaneous drainage. *Subhepatic* - The **subhepatic space** (Morison's pouch on the right) is a **common but not the most common** site for intraperitoneal abscesses. - More specifically associated with **cholecystitis**, **perforated duodenal ulcers**, or hepatobiliary surgery complications. - While dependent in the supine position, it is less dependent than the pelvis in the upright position. *Suprahepatic* - Abscesses in the **suprahepatic space** are relatively uncommon. - May occur from direct extension of liver abscesses or as complications of upper abdominal surgery. - The presence of peritoneal attachments limits widespread fluid collection in this area. *Left subphrenic space* - The **left subphrenic space** is less commonly involved than the pelvis or right subphrenic spaces. - Typically arises from complications of **splenic injury**, **pancreatitis**, **gastric perforations**, or post-splenectomy infections.
Question 7: A 40 years old male was brought emergency with severe abdominal pain. On examination, pulse rate was 112/minute and systolic BP was 80 mmHg. Chest x-ray is given below. What is the most appropriate management?
- A. Exploratory laparotomy (Correct Answer)
- B. Saline wash of stomach
- C. Intercostal tube drainage
- D. IV antibiotics
Explanation: ***Exploratory laparotomy*** - The chest x-ray shows **pneumoperitoneum (air under the diaphragm)**, which, combined with severe abdominal pain, tachycardia, and hypotension (signs of **septic shock**), is highly indicative of a **perforated viscus**. - **Emergency exploratory laparotomy** is the definitive treatment to identify and repair the perforation, control contamination, and prevent further deterioration. *Saline wash of stomach* - This procedure is typically used for gastric lavage in cases of **poisoning or drug overdose**, or to clear the stomach in preparation for endoscopy. - It does not address a viscus perforation or the widespread abdominal contamination and systemic septic response seen in this patient. *Intercostal tube drainage* - **Intercostal tube drainage** (chest tube placement) is used to drain air (pneumothorax) or fluid (pleural effusion, hemothorax, empyema) from the pleural space, not the abdominal cavity. - While there is air visible on the x-ray, it is **subdiaphragmatic (pneumoperitoneum)**, not within the pleural space, and thus a chest tube would be ineffective and inappropriate. *IV antibiotics* - **Intravenous antibiotics** are crucial for managing sepsis associated with a perforated viscus and should be administered promptly. - However, antibiotics alone are **not sufficient** to treat the underlying mechanical problem of a perforation, which requires surgical repair to prevent ongoing bacterial contamination and sepsis.
Question 8: While shaving, a 45-year-old teacher notices a marble-sized mass beneath his left ear. The mass is eventually excised, revealing which of the following benign parotid gland lesions?
- A. Cystic dilation
- B. Mikulicz's disease
- C. Warthin tumor (Correct Answer)
- D. Glandular hypertrophy, secondary to vitamin A deficiency
Explanation: ***Warthin tumor*** - **Warthin tumors** are benign, cystic tumors of the parotid gland, often presenting as a painless, soft, and mobile mass, consistent with a "marble-sized mass." - They are the second most common benign parotid neoplasm and are frequently found in older men, especially those who smoke. *Cystic dilation* - While cystic dilation can occur in the parotid gland, it is typically associated with conditions like **sialolithiasis** (salivary stones) or ductal obstruction, which would usually present with pain and swelling secondary to eating. - The description of a "marble-sized mass" without other symptoms is less typical for simple cystic dilation. *Mikulicz's disease* - Mikulicz's disease, or **IgG4-related sclerosing disease**, is a systemic condition characterized by chronic inflammation and fibrosis of exocrine glands, leading to bilateral, diffuse enlargement of various glands, including the parotid. - It usually presents with diffuse, persistent swelling, not a solitary, marble-sized mass, and is associated with elevated IgG4 levels. *Glandular hypertrophy, secondary to vitamin A deficiency* - **Glandular hypertrophy** of the parotid gland can occur due to various systemic conditions, but it is typically a diffuse, bilateral enlargement, not a discrete, unilateral mass. - While vitamin A deficiency can lead to metaplasia of glandular epithelium, it is not a direct cause of parotid gland hypertrophy or discrete mass formation.