NEET-PG 2022 — Pediatrics
9 Previous Year Questions with Answers & Explanations
What is the true statement regarding an 'at-risk baby'?
An 11-year-old child with a history of streptococcal pharyngitis presents you with fever and arthralgia. There is no past history of rheumatic heart disease or features of carditis or valvular disease. How often is 600,000 IU of benzathine penicillin recommended for prophylaxis of rheumatic heart disease?
An 8-year old child has difficulty walking and getting up from a squatting position. A muscle biopsy was done and is as shown in the image. Which of the following is true about this condition?
A child presents with recurrent chest infections and abdominal pain. There is a history of 1 blood transfusion in the past. On examination, he had icterus and mild splenomegaly. Electrophoresis shows increased HbA2, HbF, and S spike. What is the likely diagnosis?
A male child presented with arthralgia and abdominal pain. On examination, there was palpable purpura over the lower limbs. There is a past history of upper respiratory tract infection prior to the onset of presenting symptoms. Which of the following is the treatment for this condition?
A 7 – year old boy presented with abdominal pain, vomiting, oliguria, and periorbital puffiness following chemotherapy. Investigations reveal hyperuricemia, raised creatinine levels, and hyperkalemia. What is the next best step in the management of this condition ?
A 6-year-old boy came with a history of recurrent urinary tract infections. Imaging was done and showed retrograde flow of urine from the bladder into the ureters. What is the most likely diagnosis based on the imaging findings?

A 24 month child, with a weight of 11 kg, has RR of 38 / min, chest indrawing, cough and fever. Management according to IMNCI?
A blood specimen for neonatal thyroid screening is obtained on:
NEET-PG 2022 - Pediatrics NEET-PG Practice Questions and MCQs
Question 1: What is the true statement regarding an 'at-risk baby'?
- A. Mild malnutrition with weight slightly below expected norms.
- B. Socioeconomic risk due to high birth order (more than 3). (Correct Answer)
- C. Normal birth weight above the critical threshold of 2.5 kg.
- D. Severe malnutrition with weight significantly below expected norms.
Explanation: ***Socioeconomic risk due to high birth order (more than 3).*** - An **"at-risk baby"** is defined by specific criteria that identify infants vulnerable to adverse health outcomes during the neonatal and early infantile period. - **High birth order (>3)** is a recognized risk factor as per IAP (Indian Academy of Pediatrics) and WHO guidelines, primarily due to: - **Maternal depletion syndrome** (depleted maternal nutritional reserves from multiple pregnancies) - **Socioeconomic constraints** (limited resources spread across more children) - **Reduced parental attention** and care per child - Other criteria for "at-risk baby" include: birth weight <2.5 kg, preterm birth, birth asphyxia, congenital anomalies, and maternal risk factors. *Severe malnutrition with weight significantly below expected norms.* - This describes **severe acute malnutrition (SAM)** in an infant or child, which is a **nutritional disorder**, not a defining criterion of an "at-risk baby" at birth. - While malnutrition increases morbidity risk, the term "at-risk baby" specifically refers to **perinatal and neonatal risk factors** present at or around the time of birth. - SAM is a **consequence** that may develop later, rather than a defining characteristic of the "at-risk" classification. *Mild malnutrition with weight slightly below expected norms.* - **Mild malnutrition** is not a criterion for classifying a baby as "at-risk" in the standard pediatric definition. - The "at-risk baby" classification focuses on **specific measurable risk factors** (birth weight, gestational age, birth order, etc.) rather than mild nutritional deviations. *Normal birth weight above the critical threshold of 2.5 kg.* - A **normal birth weight (≥2.5 kg)** is actually a **protective factor** and indicates lower risk at birth. - This statement describes a baby who does **not meet the "at-risk" criteria** based on birth weight, though other risk factors could still be present. - Birth weight ≥2.5 kg is one indicator of adequate intrauterine growth and lower neonatal mortality risk.
Question 2: An 11-year-old child with a history of streptococcal pharyngitis presents you with fever and arthralgia. There is no past history of rheumatic heart disease or features of carditis or valvular disease. How often is 600,000 IU of benzathine penicillin recommended for prophylaxis of rheumatic heart disease?
- A. Immediately
- B. Thrice weekly lifelong
- C. Once in three weeks for 10 years or till the age of 25, whichever is longer
- D. Once in three weeks for 5 years or till the age of 18, whichever is longer (Correct Answer)
Explanation: ***Once in three weeks for 5 years or till the age of 18, whichever is longer*** - For patients with a history of **rheumatic fever** but **no carditis**, secondary prophylaxis with benzathine penicillin G is recommended for **5 years** or until **age 18**, whichever is longer. - The usual dose of benzathine penicillin G for children (under 27 kg) is **600,000 IU** intramuscularly every 3-4 weeks. *Immediately* - This option refers to the timing of initial treatment for **streptococcal pharyngitis**, not the duration or frequency of secondary prophylaxis. - Initiating antibiotic treatment immediately for acute strep throat prevents **acute rheumatic fever**, but long-term prophylaxis follows guidelines. *Thrice weekly lifelong* - This frequency is incorrect; secondary prophylaxis is typically given every **3-4 weeks**, not three times a week. - Lifelong prophylaxis is generally reserved for patients with severe **rheumatic heart disease** or those undergoing valve replacement, which is not the case here. *Once in three weeks for 10 years or till the age of 25, whichever is longer* - This duration is recommended for patients with **rheumatic fever with carditis but no residual heart disease**. - For patients with **carditis** and **residual heart disease**, prophylaxis is often extended for **10 years** or until **age 40**, or even lifelong in severe cases.
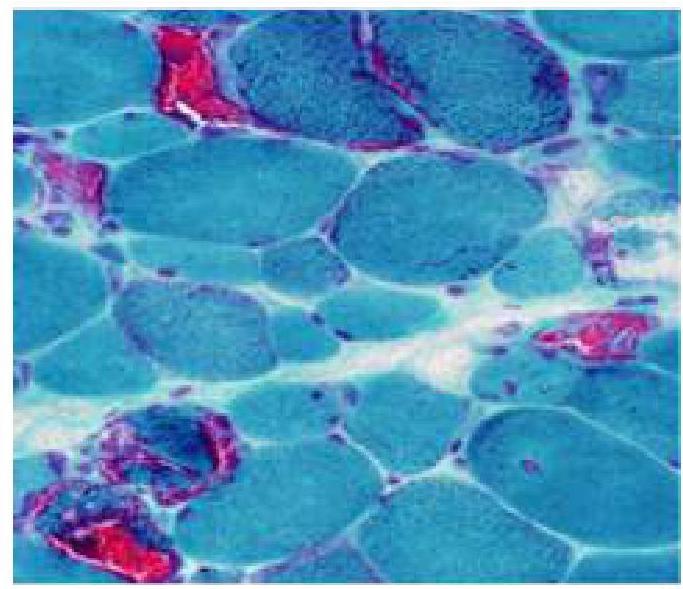
Question 3: An 8-year old child has difficulty walking and getting up from a squatting position. A muscle biopsy was done and is as shown in the image. Which of the following is true about this condition?
- A. Previous history of viral prodrome
- B. It is a mitochondrial storage disorder
- C. Early treatment has excellent prognosis
- D. Death occurs in the 3rd decade for certain types of muscular dystrophy. (Correct Answer)
Explanation: ***Death occurs in the 3rd decade for certain types of muscular dystrophy.*** - The image shows muscle fibers with varying sizes and **necrosis**, along with areas of **regeneration** and **fibrosis**, which are characteristic findings in **muscular dystrophies**, particularly Duchenne muscular dystrophy. - In **Duchenne muscular dystrophy**, patients often succumb to **respiratory or cardiac complications** by their **late teens or early twenties (3rd decade)**, making this statement true for this condition. *Previous history of viral prodrome* - A **viral prodrome** is typically associated with **acute viral myositis** or **polymyositis**, which are inflammatory conditions, not primarily genetic muscular dystrophies. - While viral infections can sometimes trigger symptoms or exacerbate underlying conditions, a direct causal link as a defining feature of muscular dystrophy is incorrect. *It is a mitochondrial storage disorder* - **Mitochondrial storage disorders** involve dysfunction of the mitochondria and can manifest as myopathies, but the histological features (ragged red fibers) and clinical presentation often differ from the classic presentation of muscular dystrophy. - The image and clinical context point towards a **dystrophinopathy**, not a primary mitochondrial disorder. *Early treatment has excellent prognosis* - Despite advances in care, **muscular dystrophies**, especially Duchenne, remain **progressive and incurable**, with treatments aimed at slowing progression and managing symptoms rather than achieving a cure or excellent prognosis. - **Early diagnosis and intervention** can improve quality of life and prolong survival but do not lead to an "excellent prognosis" in terms of disease reversal or complete functional recovery.
Question 4: A child presents with recurrent chest infections and abdominal pain. There is a history of 1 blood transfusion in the past. On examination, he had icterus and mild splenomegaly. Electrophoresis shows increased HbA2, HbF, and S spike. What is the likely diagnosis?
- A. HbC disease
- B. Sickle cell disease
- C. Aplastic anemia
- D. Sickle Beta Thalassemia (Correct Answer)
Explanation: ***Sickle Beta Thalassemia*** - The combination of **sickle cell disease manifestations** (recurrent chest infections, abdominal pain, icterus, splenomegaly) with **electrophoresis showing increased HbA2, elevated HbF, and S spike** is diagnostic of **Sickle Beta Thalassemia**. - **Increased HbA2 (>3.5%)** is the key distinguishing feature that differentiates this from pure sickle cell disease. It indicates co-inheritance of a **beta-thalassemia gene** along with the **sickle cell gene**. - Clinical presentation is similar to sickle cell disease with **vaso-occlusive crises**, **acute chest syndrome**, hemolytic anemia, and organomegaly. - The severity depends on the type: S/β⁰-thalassemia (no HbA production) is clinically more severe and similar to SS disease, while S/β⁺-thalassemia (reduced HbA) tends to be milder. *Sickle cell disease* - Pure sickle cell disease (HbSS) presents with similar clinical features: recurrent chest infections, abdominal pain, hemolysis, and splenomegaly. - However, electrophoresis would show **normal or only slightly elevated HbA2 (2-3%)**, not the increased HbA2 mentioned in this case. - The presence of significantly increased HbA2 rules out pure sickle cell disease. *HbC disease* - Patients with HbC disease typically have **mild chronic hemolytic anemia** and **splenomegaly** but usually lack severe vaso-occlusive crises. - Electrophoresis would show primarily **HbC**, not an S spike. - The clinical picture is much milder than described in this case. *Aplastic anemia* - Characterized by **pancytopenia** due to bone marrow failure, leading to fatigue, infections, and bleeding tendency. - Does not involve hemolysis, icterus, or abnormal hemoglobin variants on electrophoresis. - The electrophoresis findings completely exclude this diagnosis.
Question 5: A male child presented with arthralgia and abdominal pain. On examination, there was palpable purpura over the lower limbs. There is a past history of upper respiratory tract infection prior to the onset of presenting symptoms. Which of the following is the treatment for this condition?
- A. Azathioprine
- B. Methotrexate
- C. Cyclosporine
- D. Glucocorticoids (Correct Answer)
Explanation: ***Glucocorticoids*** - The constellation of **arthralgia**, **abdominal pain**, and **palpable purpura** following an **upper respiratory tract infection** in a child is highly suggestive of **Henoch-Schönlein purpura (HSP)**, now known as **IgA vasculitis**. - **Glucocorticoids** are indicated in HSP for severe symptoms like significant abdominal pain, gastrointestinal bleeding, or painful arthralgia, all of which this patient demonstrates. - While HSP often resolves spontaneously with supportive care, this patient's presentation with both arthralgia and abdominal pain warrants glucocorticoid therapy. *Azathioprine* - **Azathioprine** is an immunosuppressant typically used for conditions like rheumatoid arthritis, IBD, or organ transplant rejection. - It is not a first-line treatment for the acute management of **IgA vasculitis**, which typically responds to supportive care or short courses of steroids for severe symptoms. *Methotrexate* - **Methotrexate** is a disease-modifying antirheumatic drug (DMARD) used in conditions such as rheumatoid arthritis, psoriasis, and certain cancers. - It does not have a role in the acute treatment of uncomplicated **IgA vasculitis** based on the described symptoms. *Cyclosporine* - **Cyclosporine** is a potent immunosuppressant used in severe autoimmune conditions or to prevent organ rejection. - While it may be considered in very severe, refractory cases of **IgA vasculitis** with significant renal involvement, it is not the initial treatment for the symptoms presented.
Question 6: A 7 – year old boy presented with abdominal pain, vomiting, oliguria, and periorbital puffiness following chemotherapy. Investigations reveal hyperuricemia, raised creatinine levels, and hyperkalemia. What is the next best step in the management of this condition ?
- A. Hydration (Correct Answer)
- B. Probenecid
- C. Allopurinol
- D. Rasburicase
Explanation: ***Hydration*** - This patient presents with **tumor lysis syndrome (TLS)**, characterized by rapid tumor cell breakdown releasing intracellular contents (uric acid, potassium, phosphate) following chemotherapy. - **Aggressive intravenous hydration** is the **first-line and most critical initial step** in TLS management, aiming to maintain urine output at 2-3 mL/kg/hour to prevent uric acid crystal precipitation in renal tubules. - Even with oliguria present, optimizing intravascular volume and renal perfusion is essential before other interventions can be effective - without adequate hydration, rasburicase-generated allantoin cannot be excreted. - **Hydration forms the foundation** upon which all other TLS therapies depend, making it the priority "next best step." *Probenecid* - **Probenecid** is a uricosuric agent that increases renal uric acid excretion by blocking tubular reabsorption. - It is **contraindicated in tumor lysis syndrome** as it increases uric acid concentration in renal tubules, potentially worsening uric acid nephropathy and crystal formation. *Allopurinol* - **Allopurinol** is a xanthine oxidase inhibitor that prevents new uric acid formation by blocking purine metabolism. - While valuable for **prophylaxis** in high-risk patients before chemotherapy, it **does not reduce existing hyperuricemia** in established TLS. - Less effective than rasburicase for treating active, symptomatic hyperuricemia. *Rasburicase* - **Rasburicase** is a recombinant urate oxidase that rapidly converts uric acid to allantoin (5-10 times more soluble). - Highly effective for **treating established hyperuricemia** in TLS and often used in severe cases. - However, as the "next best step," **hydration must be established first** to ensure adequate renal perfusion and allow excretion of metabolites - rasburicase is typically administered **after or concurrent with** hydration initiation. - In clinical practice, both are often started together, but hydration is the foundational intervention.
Question 7: A 6-year-old boy came with a history of recurrent urinary tract infections. Imaging was done and showed retrograde flow of urine from the bladder into the ureters. What is the most likely diagnosis based on the imaging findings?
- A. Vesicoureteric reflux (VUR) (Correct Answer)
- B. Urinary bladder diverticulum (UBD)
- C. Vesicocolic fistula (VCF)
- D. Urinary bladder hernia (UBH)
Explanation: ***Vesicoureteric reflux (VUR)*** - VUR is defined by the **retrograde flow of urine from the bladder into the ureters**, which directly matches the imaging finding described - This is the **most common cause of recurrent UTIs in children**, as reflux allows bacteria to ascend from the bladder to the kidneys - Diagnosed by **voiding cystourethrogram (VCUG)**, which shows contrast refluxing into ureters during micturition - Graded from I to V based on severity; can lead to **reflux nephropathy** and renal scarring if untreated *Urinary bladder diverticulum* - An **outpouching of the bladder wall** through weakened muscle layers - May predispose to UTIs due to urinary stasis within the diverticulum, but does **not cause retrograde flow into ureters** - Imaging would show a **saccular projection** from the bladder, not ureteral filling *Vesicocolic fistula* - An **abnormal communication between bladder and colon**, typically from inflammatory bowel disease, malignancy, or trauma in adults (rare in children) - Presents with **pneumaturia (air in urine)**, fecaluria, and recurrent UTIs - Would not demonstrate **retrograde ureteral flow** on imaging *Urinary bladder hernia* - Protrusion of bladder through a **hernial defect** (inguinal, femoral, or abdominal wall) - Presents as a **reducible mass** that may increase with Valsalva - Does not cause **ureteral reflux** and has a distinct clinical and radiological presentation
Question 8: A 24 month child, with a weight of 11 kg, has RR of 38 / min, chest indrawing, cough and fever. Management according to IMNCI?
- A. Refer to a higher-level health facility for further management.
- B. Monitor at home without medical treatment.
- C. Give antibiotics (Correct Answer)
- D. Provide symptomatic treatment with antipyretics only.
Explanation: ***Give antibiotics*** - The child presents with **chest indrawing** along with cough and fever, which according to **IMNCI guidelines** classifies as **pneumonia**. - Note: RR of 38/min is **within normal limits** for a 24-month-old child (fast breathing threshold is ≥40/min for 12-59 months age group). - The diagnosis of pneumonia is based on the presence of **chest indrawing**, not fast breathing in this case. - According to **IMNCI**, pneumonia (without danger signs) should be treated with **oral antibiotics** (amoxicillin 250 mg twice daily for 5 days) at the primary care level. - The child should be followed up in 2 days and the mother advised on when to return immediately. *Refer to a higher-level health facility for further management.* - Referral is indicated for **severe pneumonia**, which requires presence of any **general danger sign** (inability to drink/breastfeed, persistent vomiting, convulsions, lethargy/unconsciousness, or stridor in calm child). - This child has **pneumonia** (not severe), so outpatient treatment with oral antibiotics is appropriate. *Monitor at home without medical treatment.* - This would be inappropriate as the child has **pneumonia** requiring antibiotic treatment. - Untreated pneumonia can rapidly progress to severe disease and is a **leading cause of child mortality** in developing countries. *Provide symptomatic treatment with antipyretics only.* - While antipyretics (paracetamol) can be given for fever, they do not treat the underlying **bacterial infection**. - Antibiotics are essential to treat pneumonia and prevent complications and mortality.
Question 9: A blood specimen for neonatal thyroid screening is obtained on:
- A. Cord blood
- B. 48 hours after birth (Correct Answer)
- C. 24 hours after birth
- D. 72 hours after birth
Explanation: ***48 hours after birth*** - Neonatal thyroid screening is optimally performed at **48-72 hours** after birth, with **48 hours** being the most practical timing in current practice. - This timing balances two important factors: avoiding the **physiological TSH surge** that occurs in the first 24 hours, while ensuring screening occurs **before early hospital discharge**. - According to **IAP (Indian Academy of Pediatrics)** and international guidelines, screening at 48 hours allows accurate detection of congenital hypothyroidism while being realistic for modern obstetric practices where most mothers are discharged within 48 hours. - The **thyroid-stimulating hormone (TSH)** levels have normalized sufficiently by 48 hours to minimize false-positive results. *Cord blood* - Cord blood is not used for routine neonatal thyroid screening because **maternal thyroid hormones** (T4 and T3) cross the placenta and can mask congenital hypothyroidism in the newborn. - It does not reflect the newborn's **independent thyroid function**, which is essential for identifying congenital disorders. *24 hours after birth* - Drawing blood at 24 hours is generally **too early** for optimal thyroid screening, as the **postnatal TSH surge** is still significant. - This timing would result in a higher rate of **false-positive results**, leading to unnecessary follow-up tests and parental anxiety. - However, if discharge occurs before 48 hours, screening at 24 hours is preferable to missing screening entirely. *72 hours after birth* - While 72 hours was traditionally recommended for thyroid screening, it is **no longer practical** in the era of early hospital discharge. - Most mothers and babies are discharged within **48 hours**, making 72-hour screening logistically difficult and risking missed screening. - Current guidelines recommend **48-72 hours OR at discharge, whichever is earlier**, making 48 hours the most optimal single timepoint.