What is the cell of origin of B-cell Acute Lymphoblastic Leukemia (B-ALL)?
Q2
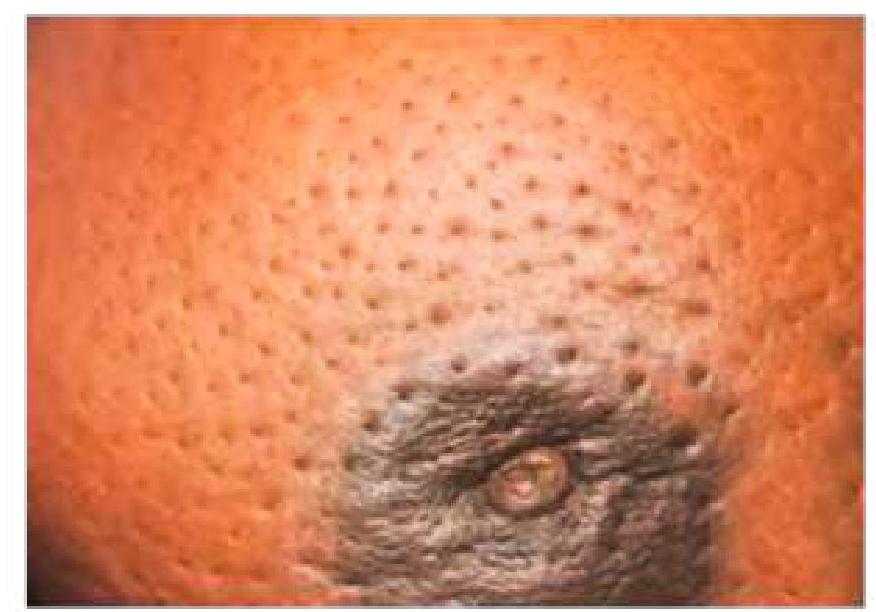
A 59-year-old lady presents with a progressive, painless lump in the breast. What is the cause of the skin change associated with breast cancer?
Q3
A middle aged male patient presents with painless slow growing neck swelling. On examination, lymph nodes are positive. Surgery is done and biopsy is shown in the image below. Which of the following is false regarding the HPE findings?
NEET-PG 2022 - Pathology NEET-PG Practice Questions and MCQs
Question 1: What is the cell of origin of B-cell Acute Lymphoblastic Leukemia (B-ALL)?
A. T cells
B. Immature B cells (Correct Answer)
C. Immature T cells
D. Both T & B cells
Explanation: ***Immature B cells***
- B acute lymphoblastic leukemia (B ALL) is primarily derived from the **malignant transformation of precursor B lymphocytes** [1].
- The disease is characterized by the presence of **immature B cell blasts** in the bone marrow and peripheral blood [1].
*T cells*
- T cells are involved in a different lineage of leukemia known as T-ALL, not B ALL [1].
- The pathophysiology of B ALL specifically relates to **B cell precursors**, not T cell involvement.
*Both T & B cells*
- This option is incorrect as B ALL specifically originates from **B cell lineage**, and T cells are unrelated to its pathogenesis [1].
- The presence of both T and B cells together characterizes mixed lineage leukemias, which is not the case here.
*Immature T cells*
- Immature T cells are precursors for **T acute lymphoblastic leukemia (T-ALL)**, not for B ALL [1].
- B ALL does not involve T cell precursors; the focus is solely on **immature B cells** [1].
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 596-600.
Question 2: A 59-year-old lady presents with a progressive, painless lump in the breast. What is the cause of the skin change associated with breast cancer?
A. Infiltration of subdermal lymphatics (Correct Answer)
B. Infiltration of the lactiferous duct
C. Involvement of Cooper’s ligament
D. Spread of the tumor to the anterior chest wall
Explanation: ***Infiltration of subdermal lymphatics***
- The skin change described often refers to **peau d'orange**, which is caused by the **blockage of superficial lymphatic vessels** by tumor cells [1].
- This lymphatic obstruction leads to **edema** and dimpling of the skin, resembling an orange peel [1].
*Infiltration of the lactiferous duct*
- While cancer can arise in or infiltrate lactiferous ducts, this primarily causes symptoms like **nipple discharge**, inversion, or a palpable mass.
- It does not directly explain the specific **skin dimpling** or **peau d'orange** appearance.
*Involvement of Cooper's ligament*
- Involvement of **Cooper's ligaments** (suspensory ligaments of the breast) can cause skin dimpling or retraction [1].
- However, the image depicts widespread **peau d'orange**, which is more commonly associated with lymphatic involvement than direct ligamentous retraction [1].
*Spread of the tumor to the anterior chest wall*
- Tumor extension to the **anterior chest wall** signifies advanced disease and can cause **fixation of the breast** to underlying structures or skin ulceration [2].
- This typically results in **immobility of the breast** or an ulcerated lesion, not the widespread edematous and dimpled appearance of **peau d'orange**.
**References:**
[1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 453-454.
[2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 456-457.
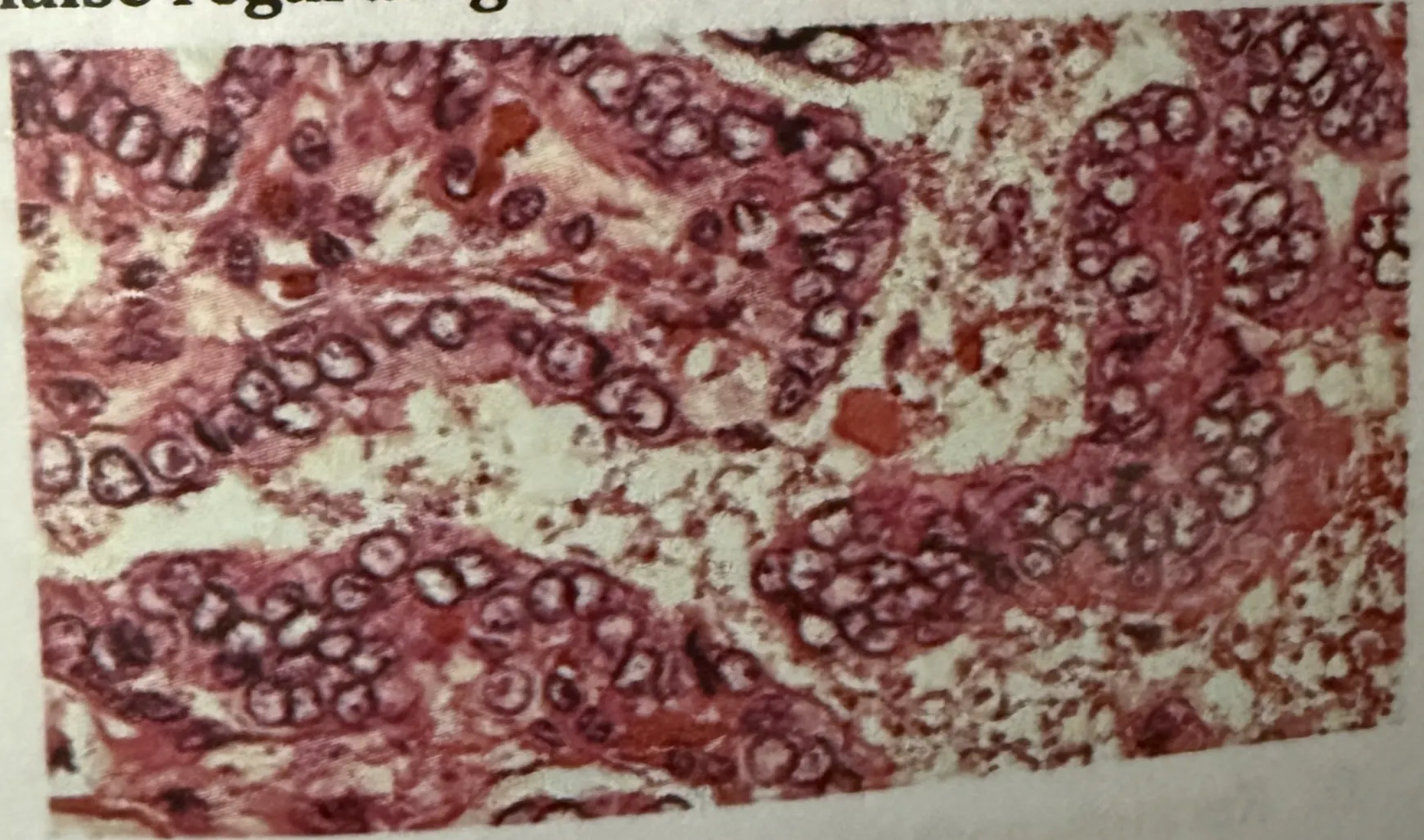
Question 3: A middle aged male patient presents with painless slow growing neck swelling. On examination, lymph nodes are positive. Surgery is done and biopsy is shown in the image below. Which of the following is false regarding the HPE findings?
A. Spread is through lymphatics
B. Nuclear features are the characteristic of this tumor
C. FNAC is not diagnostic (Correct Answer)
D. It has excellent prognosis
Explanation: ***Fine needle aspiration cytology (FNAC) is not diagnostic***
- FNAC can often provide significant insights, but in cases of **specific malignancies** or certain lesions, it may not yield definitive diagnoses [1].
- Diagnostic challenges arise as **cellular architecture** or certain **nuclear features** may not be appreciated in FNAC samples [1].
*It spreads quickly via lymphatics*
- This condition can indeed spread via lymphatics, making it **aggressive** in nature [1].
- **Lymphatic spread** is a common pathway for many head and neck conditions, particularly malignancies [1].
*Excellent prognosis is associated with this condition*
- While some conditions may have favorable prognoses, many midline neck lesions can have **serious implications** depending on their nature [1].
- Prognosis often varies widely and may not always be classified as **excellent** based solely on initial presentation [1].
*Nuclear characteristics are used for the identification*
- Nuclear morphology is critical for identifying various **neoplastic conditions**, aiding in differentiation from benign lesions [1][2].
- Many pathologies, especially those involving **malignancy**, rely heavily on **nuclear features** for accurate diagnosis [1][2].
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1101-1102.
[2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1100-1101.