All (140)Anatomy (8)Anesthesiology (2)Biochemistry (10)Community Medicine (10)Dental (3)Dermatology (5)ENT (3)Forensic Medicine (8)Internal Medicine (22)Microbiology (10)Obstetrics and Gynecology (17)Ophthalmology (2)Orthopaedics (3)Pathology (5)Pediatrics (7)Pharmacology (8)Physiology (3)Psychiatry (1)Psychiatry (2)Radiology (2)Surgery (9)
Q81
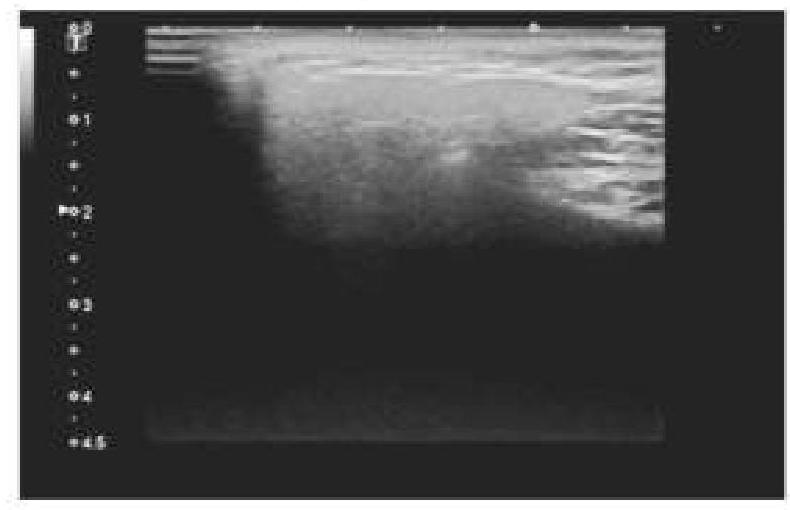
A 45-year-old patient complained of pain on one side of the neck. She is afraid of eating food as it worsens the pain. An ultrasound of the salivary glands is shown below. What is the most likely diagnosis?