All (139)Anatomy (8)Anesthesiology (2)Biochemistry (10)Community Medicine (10)Dental (3)Dermatology (5)ENT (3)Forensic Medicine (7)Internal Medicine (22)Microbiology (10)Obstetrics and Gynecology (17)Ophthalmology (2)Orthopaedics (3)Pathology (5)Pediatrics (7)Pharmacology (8)Physiology (3)Psychiatry (1)Psychiatry (2)Radiology (2)Surgery (9)
Q71
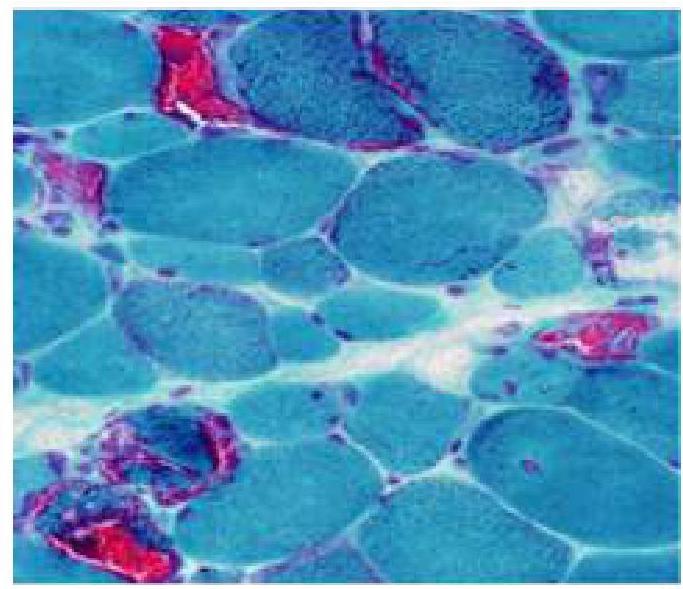
An 8-year old child has difficulty walking and getting up from a squatting position. A muscle biopsy was done and is as shown in the image. Which of the following is true about this condition?