All (140)Anatomy (8)Anesthesiology (2)Biochemistry (10)Community Medicine (10)Dental (3)Dermatology (5)ENT (3)Forensic Medicine (8)Internal Medicine (22)Microbiology (10)Obstetrics and Gynecology (17)Ophthalmology (2)Orthopaedics (3)Pathology (5)Pediatrics (7)Pharmacology (8)Physiology (3)Psychiatry (1)Psychiatry (2)Radiology (2)Surgery (9)
Q11
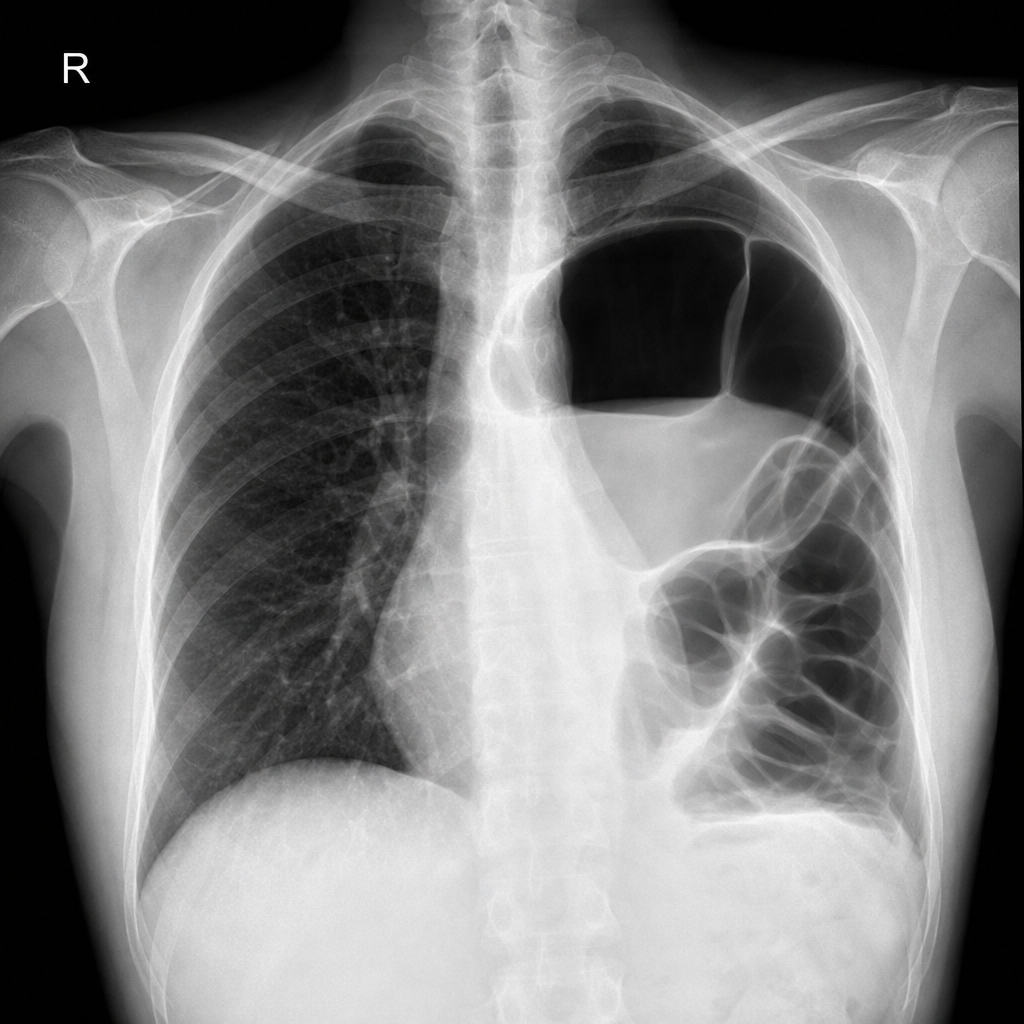
The shown radiograph indicates which condition?