All (139)Anatomy (8)Anesthesiology (2)Biochemistry (10)Community Medicine (10)Dental (3)Dermatology (5)ENT (3)Forensic Medicine (7)Internal Medicine (22)Microbiology (10)Obstetrics and Gynecology (17)Ophthalmology (2)Orthopaedics (3)Pathology (5)Pediatrics (7)Pharmacology (8)Physiology (3)Psychiatry (1)Psychiatry (2)Radiology (2)Surgery (9)
Q121
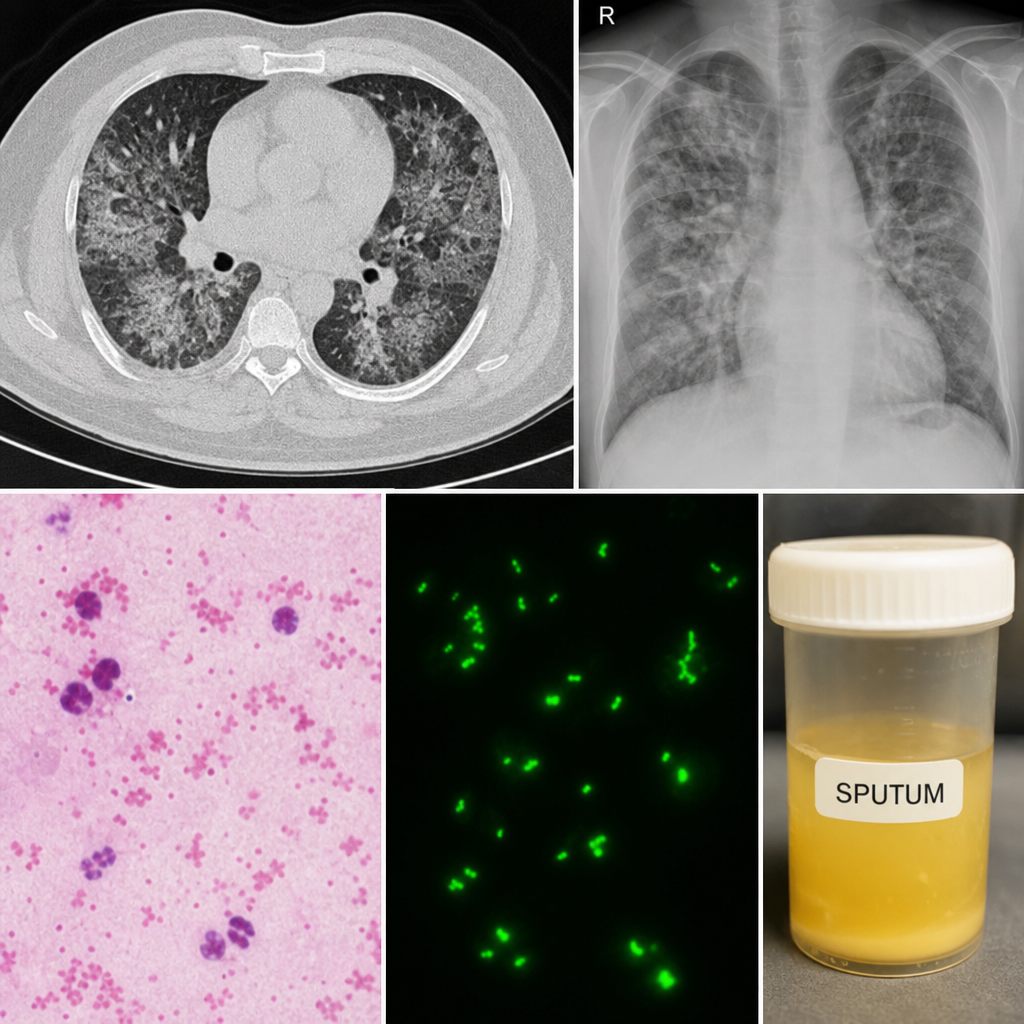
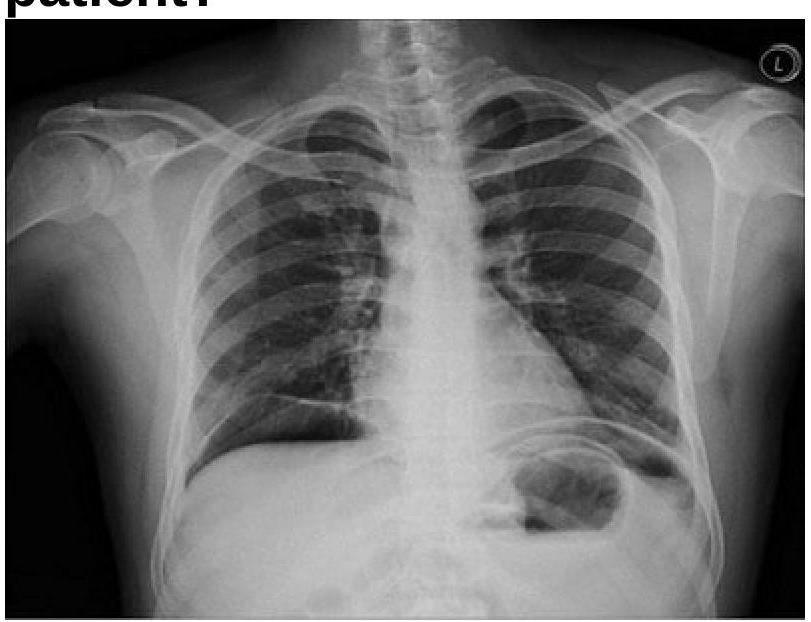
A 40-year-old male presented with fever, cough with expectoration and shoness of breath, mild confusion for 1 week. Patient gave history of shower in a public washroom 10 days back. Patient also repoed some episodes of diarrhoea. Sputum sample was taken. And gram staining and direct fluorescent antibody test were done. CT Scan Which of the following lab findings would be most commonly found: -