NEET-PG 2022 — Obstetrics and Gynecology
20 Previous Year Questions with Answers & Explanations
A multigravida at term with a transverse lie and hand prolapse, along with a fetal heart rate of 140/min, is best managed by:
A woman with two children presents with galactorrhea and amenorrhea for one year. The most probable diagnosis is:
When in labor, a diagnosis of occipito-posterior presentation is made. The most appropriate management would be:
After 3rd stage of labour and expulsion of placenta, the patient is bleeding heavily. Ideal management would include all except:
Identify the type of hymen.
A 24 year old lactating female with an 18 month old child comes with a history of irregular, heavy bleeding seeking contraceptive advice. Which is the contraceptive of choice?
A woman with an obstetric score of G2P1 comes to the clinic at 14 weeks of gestation for her antenatal checkup. A uterine artery doppler was suggested by the doctor. What would it detect?
A pregnant patient, with a history of classical cesarean section in view of fetal growth retardation in the previous pregnancy, presents to you. She is currently at 35 weeks of gestation with breech presentation. What is the next step in management?
A primigravida presents to the labor room at 40 weeks of gestation with lower abdominal pain. She has been in labor for 3 hours. Which of the following will determine if she is in active labor?
A woman at 26 weeks of gestation presents for routine evaluation. On examination, fundal height corresponds to 24 weeks. Ultrasonography revealed decreased amniotic fluid. Which of the following conditions would have led to this presentation?
NEET-PG 2022 - Obstetrics and Gynecology NEET-PG Practice Questions and MCQs
Question 1: A multigravida at term with a transverse lie and hand prolapse, along with a fetal heart rate of 140/min, is best managed by:
- A. External cephalic version
- B. Cesarean delivery (Correct Answer)
- C. Breech delivery
- D. Internal podalic version
Explanation: ***Cesarean delivery*** - A **transverse lie** at term is a contraindication to vaginal delivery, as the fetus cannot pass through the birth canal in this orientation. - The presence of **hand prolapse** further complicates the situation, increasing the risk of umbilical cord prolapse and fetal distress, making cesarean section the safest option. *External cephalic version* - This procedure is performed to change a **breech or transverse lie** to a cephalic presentation, but it is typically done *before* term, usually between 36-37 weeks. - It is contraindicated once labor has started or with **membrane rupture** and fetal parts prolapsed, as is implied by hand prolapse in this term patient. *Breech delivery* - Breech delivery involves the fetus presenting buttocks or feet first, which is not the case here; the presentation is **transverse lie** and **hand prolapse**. - While some breech deliveries can be attempted vaginally under specific circumstances, this patient's presentation makes it an inappropriate option. *Internal podalic version* - This procedure involves changing a **transverse lie** to a **breech presentation** by internal manipulation, often performed in cases of twin delivery for the second twin or in specific scenarios of malpresentation in earlier gestations. - It is rarely performed for a single fetus at term due to risks for both mother and fetus, especially with a **term fetus** and **hand prolapse**.
Question 2: A woman with two children presents with galactorrhea and amenorrhea for one year. The most probable diagnosis is:
- A. Ectopic pregnancy
- B. Prolactinoma (Correct Answer)
- C. Pituitary apoplexy
- D. Hypothalamic dysfunction
Explanation: ***Prolactinoma*** - The classic presentation of **galactorrhea** (milk production unrelated to pregnancy or breastfeeding) and **amenorrhea** (absence of menstruation) in a non-pregnant woman strongly suggests hyperprolactinemia, most commonly due to a **prolactin-secreting pituitary adenoma** (prolactinoma). - High prolactin levels can inhibit GnRH pulsatility from the hypothalamus, leading to decreased LH and FSH secretion, which in turn causes **anovulation** and thus amenorrhea. *Ectopic pregnancy* - This condition presents with symptoms like **abdominal pain**, vaginal bleeding, and a **positive pregnancy test**, which are not mentioned here. - While an ectopic pregnancy is a cause of amenorrhea, it does not typically cause galactorrhea. *Pituitary apoplexy* - This is an acute, life-threatening condition caused by hemorrhage or infarction of the pituitary gland, presenting with **sudden severe headache**, visual disturbances, and altered mental status. - While it can affect pituitary function, its acute onset and severe symptoms are inconsistent with the one-year history of galactorrhea and amenorrhea. *Hypothalamic dysfunction* - Although hypothalamic dysfunction can cause amenorrhea due to impaired GnRH release, it typically presents with **low or normal prolactin levels**, not elevated prolactin causing galactorrhea. - Conditions like **functional hypothalamic amenorrhea** (due to stress, excessive exercise, or low body weight) would involve a different hormonal profile.
Question 3: When in labor, a diagnosis of occipito-posterior presentation is made. The most appropriate management would be:
- A. Emergency CS
- B. Wait and watch for progress of labor (Correct Answer)
- C. Early rupture of membranes
- D. Start oxytocin drip
Explanation: ***Wait and watch for progress of labor*** - Many **occipito-posterior (OP) presentations** will spontaneously rotate to an occipito-anterior (OA) position with ongoing contractions, especially in multiparous women. - Close monitoring of fetal well-being and labor progress is essential, but immediate intervention is not always required. *Emergency CS* - An emergency cesarean section is typically reserved for cases where there is **fetal distress**, **failure to progress** after a reasonable period of observation, or other clear obstetric indications. - An OP presentation alone, without complications, does not warrant an immediate CS. *Early rupture of membranes* - While sometimes used to evaluate cervical dilation or apply a fetal scalp electrode, **early artificial rupture of membranes (AROM)** in OP presentation is not a definitive management strategy. - It may even increase the risk of cord prolapse or ascending infection without necessarily expediting rotation. *Start oxytocin drip* - **Oxytocin augmentation** may be considered if contractions are inadequate and labor is prolonged, but it's not the first-line management for OP presentation itself. - It should only be initiated after assessing the power, passage, and passenger, and ensuring there are no contraindications to augmentation.
Question 4: After 3rd stage of labour and expulsion of placenta, the patient is bleeding heavily. Ideal management would include all except:
- A. Check for laceration of labia
- B. Uterine massage and I/V oxytocin
- C. APGAR scoring (Correct Answer)
- D. Check for placenta in uterus
Explanation: ***APGAR scoring*** - **APGAR scoring** assesses the newborn's health immediately after birth and is not a management step for **postpartum hemorrhage**. - This intervention would divert critical attention from the mother's life-threatening bleeding. *Check for placenta in uterus* - **Retained placental fragments** are a common cause of **postpartum hemorrhage**, obstructing uterine contraction. - Checking for and removing any retained placenta is a crucial and immediate management step to control bleeding. *Check for laceration of labia* - **Lacerations of the birth canal**, including the labia, vagina, or cervix, can cause significant bleeding after delivery, even with a well-contracted uterus. - Identifying and repairing these lacerations is an essential part of managing **postpartum hemorrhage not due to atony**. *Uterine massage and I/V oxytocin* - **Uterine atony** (failure of the uterus to contract) is the most common cause of **postpartum hemorrhage**. - **Uterine massage** helps stimulate contraction, and **intravenous oxytocin** is a uterotonic agent used to promote uterine contraction and reduce bleeding.
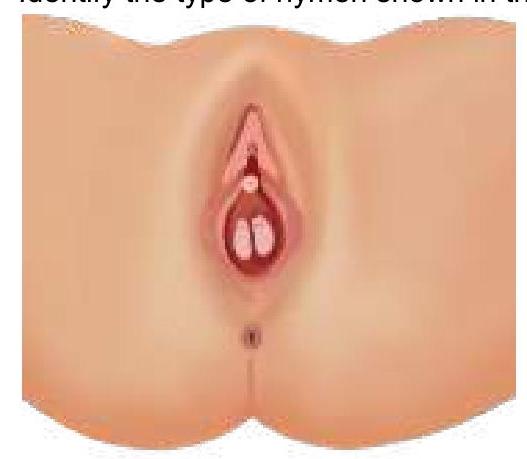
Question 5: Identify the type of hymen.
- A. Imperforate hymen
- B. Semilunar hymen
- C. Septate hymen (Correct Answer)
- D. Annular hymen
Explanation: ***Septate hymen*** - The image clearly displays a **band of tissue** running across the hymenal opening, dividing it into two smaller openings, which is characteristic of a **septate hymen**. - This type of hymen can sometimes interfere with menstruation or intercourse and may require surgical correction. *Imperforate hymen* - An **imperforate hymen** completely covers the vaginal opening, with no perforations for menstrual flow. - This typically presents at menarche with **abdominal pain** and a bulging hymen due to retained menstrual blood (hematocolpos). *Semilunar hymen* - A **semilunar hymen** is incomplete, forming a crescent shape at the posterior aspect of the vaginal opening. - This is a common and normal variant, usually not causing any clinical issues. *Annular hymen* - An **annular hymen** is characterized by a circular opening in the center, encircled by hymenal tissue, appearing like a ring. - This is a common hymenal configuration and usually allows for normal menstrual flow.
Question 6: A 24 year old lactating female with an 18 month old child comes with a history of irregular, heavy bleeding seeking contraceptive advice. Which is the contraceptive of choice?
- A. Progestin-only pill (Correct Answer)
- B. Copper IUD
- C. Progestin-only injection
- D. Combined oral contraceptive pill
Explanation: ***Progestin-only pill*** - The **progestin-only pill (POP)** is the contraceptive of choice for lactating women because it does not affect **breast milk supply** or composition. - It works by thickening cervical mucus and thinning the **endometrium**, which can help reduce heavy bleeding and provide effective contraception. *Copper IUD* - While the **copper IUD** is a highly effective contraceptive, it is known to potentially increase **menstrual bleeding** and cramping. - Given the patient's history of **heavy bleeding**, a copper IUD might worsen her symptoms. *Progestin-only injection* - **Progestin-only injections** like DMPA are highly effective and safe for lactating women, but they can cause **irregular bleeding patterns** initially and are associated with a slower return to fertility. - While an option, the **progestin-only pill** offers more immediate control over menstrual patterns and easier discontinuation if side effects are problematic. *Combined oral contraceptive pill* - **Combined oral contraceptive pills (COCs)** contain both estrogen and progestin. Estrogen can negatively impact **milk production** and may not be suitable for breastfeeding mothers, especially in the first 6 months postpartum. - COCs are generally avoided in lactating women until breastfeeding is well-established or after 6 months to prevent interference with **lactation**.
Question 7: A woman with an obstetric score of G2P1 comes to the clinic at 14 weeks of gestation for her antenatal checkup. A uterine artery doppler was suggested by the doctor. What would it detect?
- A. Risk of early-onset preeclampsia (Correct Answer)
- B. Risk of late-onset preeclampsia
- C. Risk of placenta accreta
- D. Fetal growth restriction risk
Explanation: **Risk of early-onset preeclampsia** - **Uterine artery Doppler** at 11-14 weeks of gestation is used to screen for **preeclampsia risk**, particularly **early-onset preeclampsia**, which is associated with impaired placental development. - An increased **pulsatility index (PI)** or presence of **bilateral notching** in the uterine arteries indicates high resistance to blood flow, suggesting a higher risk of developing this condition. *Risk of late-onset preeclampsia* - While uterine artery Doppler can indicate a general risk for preeclampsia, its predictive value is significantly lower for **late-onset preeclampsia** (after 34 weeks). - Late-onset preeclampsia often has different underlying causes, not solely related to abnormal **trophoblast invasion** detectable by early Doppler. *Risk of placenta accreta* - **Placenta accreta** is typically associated with previous **cesarean sections** or other uterine surgeries, leading to abnormal placental implantation. - It is diagnosed by the absence of a clear retroplacental hypoechoic zone and features such as **lacunae** on **ultrasound**, not primarily by uterine artery Doppler. *Fetal growth restriction risk* - Uterine artery Doppler at 11-14 weeks can offer some indication of **fetal growth restriction (FGR)** risk, particularly if severe and related to **placental insufficiency**. - However, the primary surveillance for FGR later in pregnancy often involves **umbilical artery Doppler** and fetal biometry, not solely early uterine artery Doppler.
Question 8: A pregnant patient, with a history of classical cesarean section in view of fetal growth retardation in the previous pregnancy, presents to you. She is currently at 35 weeks of gestation with breech presentation. What is the next step in management?
- A. Cesarean section at 37 weeks (Correct Answer)
- B. Advice USG and visit after 2 weeks
- C. Internal podalic version followed by vaginal delivery
- D. External cephalic version at 36 weeks
Explanation: ***Cesarean section at 37 weeks*** - A history of **classical cesarean section** is an absolute contraindication to vaginal birth due to the high risk of **uterine rupture**. - Performing the cesarean section at 37 weeks, rather than waiting longer, minimizes the risk of spontaneous labor and rupture while ensuring fetal maturity. *Advice USG and visit after 2 weeks* - This option does not address the critical risk of **uterine rupture** due to the previous classical cesarean section. - Delaying definitive management by two weeks could increase the risk of spontaneous labor and associated complications. *Internal podalic version followed by vaginal delivery* - An **internal podalic version** is a procedure used to change fetal lie during labor, typically for the second twin, and it is **contraindicated** with a previous classical cesarean due to rupture risk. - Given the previous classical incision, a **vaginal delivery is unsafe** and should not be attempted. *External cephalic version at 36 weeks* - **External cephalic version (ECV)** is generally contraindicated in patients with a history of a **classical cesarean section** due to the increased risk of uterine rupture. - Even if successful, the patient would still require a cesarean section for delivery given the previous uterine scar.
Question 9: A primigravida presents to the labor room at 40 weeks of gestation with lower abdominal pain. She has been in labor for 3 hours. Which of the following will determine if she is in active labor?
- A. Fetal head 5/5 palpable on abdominal examination
- B. Two contractions lasting for 10 seconds in 10 minutes
- C. Rupture of membranes
- D. Cervical dilatation of 6 cm or more with regular contractions (Correct Answer)
Explanation: ***Cervical dilatation of 6 cm or more with regular contractions*** - Active labor is officially defined by **cervical dilatation of 6 cm or more** according to the ACOG and SMFM 2014 consensus guidelines, which redefined the labor curve based on the Consortium on Safe Labor study. - This represents a shift from the traditional Friedman curve definition of 4 cm, recognizing that **significant progressive cervical change** with regular uterine contractions is the hallmark of active labor. - Complete effacement typically occurs during the latent phase, and while regular contractions accompany active labor, **cervical dilatation ≥6 cm is the primary diagnostic criterion**. *Fetal head 5/5 palpable on abdominal examination* - This finding indicates a **high fetal head** that is not engaged (0/5 of the head has entered the pelvis), which does not determine whether active labor has begun. - **Fetal station and engagement** are important for assessing labor progression and potential for cephalopelvic disproportion, but are not the primary criteria for diagnosing active labor. *Two contractions lasting for 10 seconds in 10 minutes* - These contractions are **infrequent and very short**, more characteristic of latent labor or Braxton Hicks contractions. - Active labor typically involves **3-5 contractions in 10 minutes, each lasting 45-60 seconds**, with sufficient intensity to cause progressive cervical change. *Rupture of membranes* - **Rupture of membranes (ROM)**, whether spontaneous or artificial, is an important event but does not by itself indicate active labor. - A woman can have ROM in the **latent phase** or even before labor begins (prelabor ROM or PROM), and **cervical dilatation remains the primary determinant** of active labor.
Question 10: A woman at 26 weeks of gestation presents for routine evaluation. On examination, fundal height corresponds to 24 weeks. Ultrasonography revealed decreased amniotic fluid. Which of the following conditions would have led to this presentation?
- A. Renal agenesis (Correct Answer)
- B. Tracheoesophageal fistula
- C. Cardiac abnormalities
- D. Ureteral stricture
Explanation: ***Renal agenesis*** - **Renal agenesis** directly leads to **oligohydramnios** (decreased amniotic fluid) because fetal urine is the primary contributor to amniotic fluid volume after 20 weeks of gestation. - This reduction in amniotic fluid subsequently causes a **smaller fundal height** than expected for gestational age. *Tracheoesophageal fistula* - A **tracheoesophageal fistula** is primarily associated with **polyhydramnios** (excessive amniotic fluid) due to the fetus's inability to properly swallow amniotic fluid. - It would not lead to decreased amniotic fluid or a reduced fundal height. *Cardiac abnormalities* - **Cardiac abnormalities** can cause various fetal complications but are not typically a direct cause of **oligohydramnios**. - While severe cardiac issues can indirectly impact fetal growth, they usually do not lead to a significant reduction in amniotic fluid volume. *Ureteral stricture* - A **ureteral stricture** would impair urine flow from the kidney to the bladder, causing **hydronephrosis** of the affected kidney. - While it affects the renal system, if the other kidney is functioning, it generally would not lead to widespread **oligohydramnios** or a significantly reduced fundal height.