All SubjectsAnatomy (8)Anesthesiology (2)Biochemistry (10)Community Medicine (10)Dental (3)Dermatology (5)ENT (3)Forensic Medicine (7)Internal Medicine (22)Microbiology (10)Obstetrics and Gynecology (17)Ophthalmology (2)Orthopaedics (3)Pathology (5)Pediatrics (7)Pharmacology (8)Physiology (3)Psychiatry (1)Psychiatry (2)Radiology (2)Surgery (9)
Q11
A patient diagnosed to be HIV-positive was started on highly active antiretroviral therapy (HAART). Which of the following can be used to monitor treatment efficacy?
Q12
A male patient presents to the emergency department. The arterial blood gas report is as follows: pH, 7.2; pCO2, 81 mmHg; and HCO3, 40 meq/L. Which of the following is the most likely diagnosis?
Q13
A woman presents to you with fever, arthralgia, ulcers, fatigue for the past six months, and new-onset hematuria. Urine examination reveals RBC casts and proteinuria. What is the likely diagnosis?
Q14
A patient with diabetes mellitus for the past 5 years presents with vomiting and abdominal pain. She is non-compliant with medication and appears dehydrated. Investigations revealed a blood sugar value of 500 mg/dl and the presence of ketone bodies. What is the next best step in management of this patient?
Q15
A patient on anti-depressants presented to you with hypotension. An ECG was done, which showed wide QRS complexes and right axis deviation. How will you manage this patient?
Q16
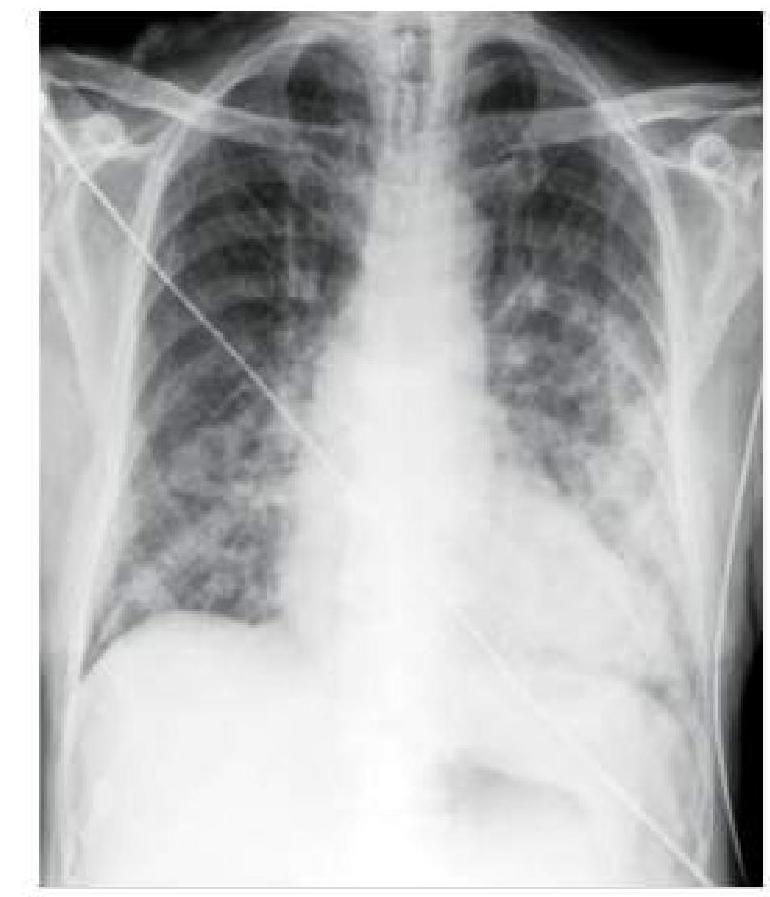
A hypertensive patient who is non-compliant with medication presents to you with sudden onset breathlessness. A chest x-ray was done, which is shown below. How will you manage this patient?
Q17
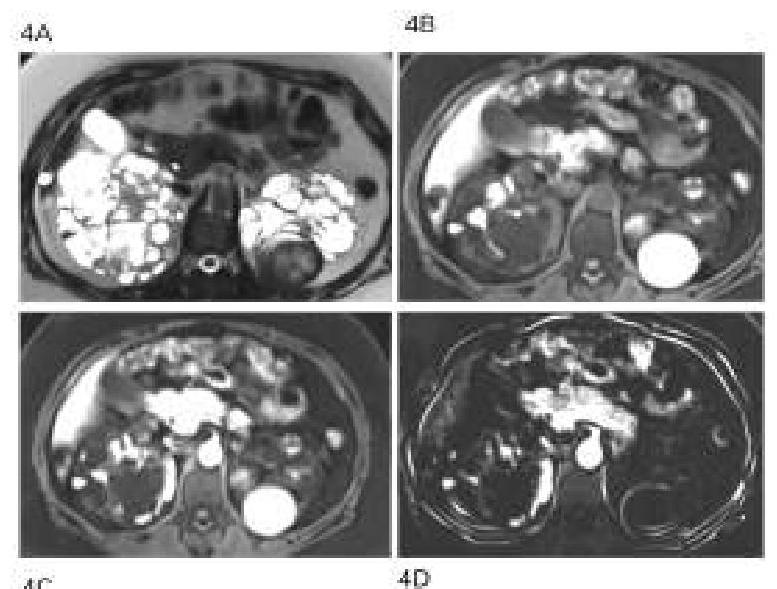
A 40-year-old man with a known case of hypertension presented with multiple episodes of hematuria and loin pain. His elder brother passed away due to a stroke at the age of 40. What is the probable diagnosis based on the clinical presentation?
Q18
Which of the following is the MOST common complication of untreated hypertension?
Q19
What is the initial treatment for most patients with growth hormone-secreting pituitary adenoma?
Q20
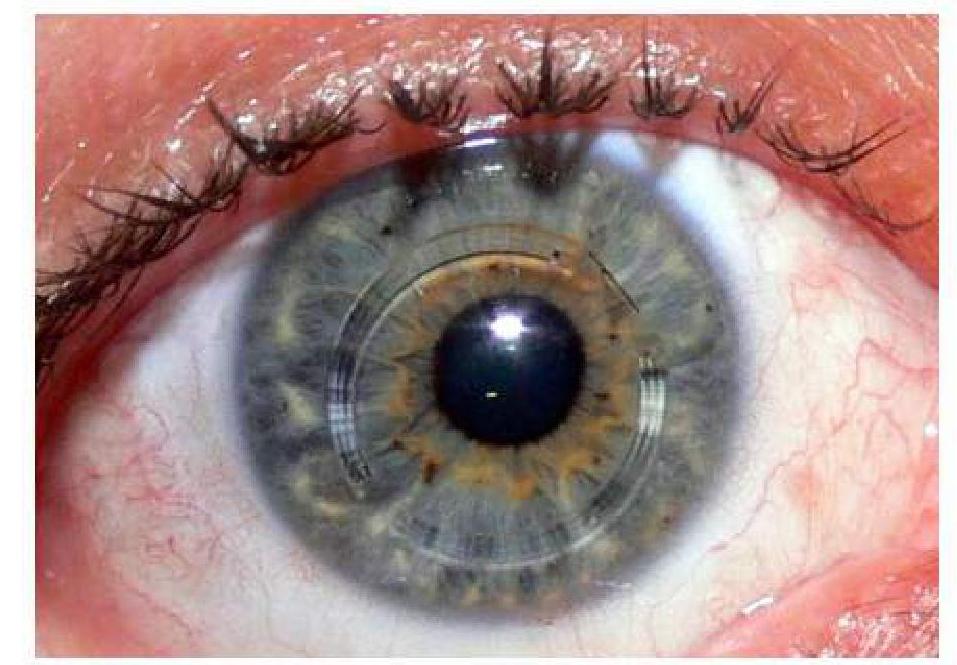
A 40-year-old woman with rheumatoid arthritis presents with eye pain and redness. Examination reveals scleritis. What is the most likely associated systemic complication?