NEET-PG 2022 — Internal Medicine
22 Previous Year Questions with Answers & Explanations
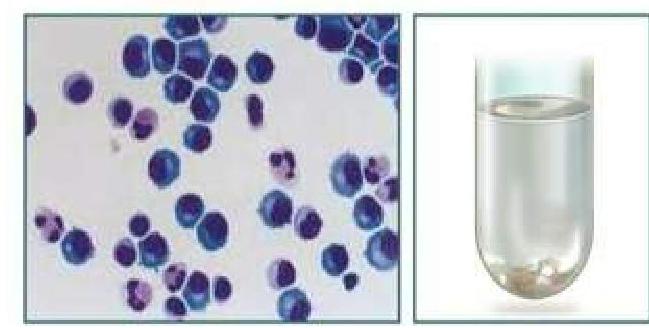
Which of the following is typically seen in cerebrospinal fluid (CSF) in tubercular meningitis?
Which one of the following is an autosomal recessive disorder?
Which of the following is not seen in MEN 2B syndrome?
A patient presents to you with fever, night sweats, ptosis, and bilateral facial nerve palsy. Investigations showed leukocytosis and bilateral hilar lymphadenopathy. Which of the following is the most likely diagnosis?
A patient with a history of chronic liver disease presents with abdominal distension, jaundice, and pruritis. Ascitic fluid analysis revealed a neutrophil count >650 per cubic mm. What is the most likely diagnosis?

A patient presents with a unilateral throbbing headache, photophobia, and excessive lacrimation. He also complains of hemifacial pain on the clenching of teeth. On examination, pupillary reaction, light reflex, and accommodation reflex are normal. Which of the following marked nerves is most likely involved in the above scenario?
A patient presents to you with an irregularly irregular pulse of 120/minutes and a pulse deficit of 20. Which of the following would be the jugular venous pressure (JVP) finding?

A woman presents to you with fever, arthralgia, ulcers, fatigue for the past six months, and new-onset hematuria. Urine examination reveals RBC casts and proteinuria. What is the likely diagnosis?
A male patient diagnosed with tuberculosis took complete treatment. Sputum examination was done after the completion of the intensive and the continuation phases. It was found to be negative. What is the status of the patient?
A woman with recurrent diarrhea is prescribed a broad-spectrum antibiotic. Which of the following statements is not true regarding Clostridium difficile infection?
NEET-PG 2022 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 1: Which of the following is typically seen in cerebrospinal fluid (CSF) in tubercular meningitis?
- A. Low sugar
- B. High protein
- C. Low opening pressure (Correct Answer)
- D. Lymphocytic Pleocytosis
Explanation: ***Low opening pressure*** - While **elevated opening pressure** is common in tubercular meningitis due to inflammation and impaired CSF absorption, **low opening pressure** is not a typical finding. - Low opening pressure can occur with conditions like **CSF leak** or **spinal tap headache**, which are not directly characteristic of tubercular meningitis. *Low sugar* - **Low CSF glucose** (hypoglycorrhachia) is highly characteristic of bacterial and tubercular meningitis, as the bacteria or mycobacteria consume glucose. - The **CSF-to-blood glucose ratio** is typically less than 0.4 in tubercular meningitis. *High protein* - **Elevated CSF protein** is a consistent finding in tubercular meningitis, resulting from inflammation, increased vascular permeability, and breakdown of the blood-brain barrier. - Protein levels often range from **100-500 mg/dL** or even higher. *Lymphocytic Pleocytosis* - **Lymphocytic pleocytosis** (increased lymphocytes in CSF) is a hallmark of tubercular meningitis, although early stages might show a mixed cellular response. - The cell count typically ranges from **100-500 cells/µL**, predominantly lymphocytes.
Question 2: Which one of the following is an autosomal recessive disorder?
- A. Cystic fibrosis (Correct Answer)
- B. Huntington's disease
- C. Marfan syndrome
- D. Neurofibromatosis type 1
Explanation: ***Cystic fibrosis*** - **Cystic fibrosis** is caused by mutations in the **CFTR gene**, leading to defective **chloride channel** function. - It is an **autosomal recessive disorder**, meaning an individual must inherit two copies of the mutated gene (one from each parent) to be affected. *Huntington's disease* - **Huntington's disease** is an **autosomal dominant disorder** caused by a mutation in the HTT gene. - Only one copy of the mutated gene is sufficient to cause the disease, resulting in progressive neurodegeneration. *Marfan syndrome* - **Marfan syndrome** is an **autosomal dominant disorder** affecting connective tissue, caused by mutations in the FBN1 gene. - It results in skeletal, ocular, and cardiovascular abnormalities due to defective **fibrillin-1**. *Neurofibromatosis type 1* - **Neurofibromatosis type 1** is an **autosomal dominant disorder** caused by mutations in the NF1 gene. - It is characterized by multiple neurofibromas, café-au-lait macules, and Lisch nodules.
Question 3: Which of the following is not seen in MEN 2B syndrome?
- A. Mucosal neuroma
- B. Marfanoid habitus
- C. Parathyroid adenoma (Correct Answer)
- D. Megacolon
Explanation: ***Parathyroid adenoma*** - **Parathyroid adenomas**, leading to hyperparathyroidism, are characteristic of **MEN 2A syndrome**, not MEN 2B [1]. - While both MEN 2A and 2B involve mutations in the **RET proto-oncogene**, the specific clinical manifestations differ significantly. *Megacolon* - **Megacolon** (due to intestinal ganglioneuromatosis) is a recognized feature of **MEN 2B syndrome**. - This condition involves abnormal nerve ganglion cells in the intestine, leading to motility issues. *Mucosal neuroma* - **Mucosal neuromas** on the tongue, lips, and eyelids are a hallmark clinical sign of **MEN 2B syndrome**. - These benign growths are often one of the earliest and most recognizable features. *Marfanoid habitus* - **Marfanoid habitus**, characterized by a tall, slender build with long limbs and arachnodactyly, is a common physical finding in **MEN 2B syndrome**. - This connective tissue abnormality helps distinguish MEN 2B from other MEN syndromes.
Question 4: A patient presents to you with fever, night sweats, ptosis, and bilateral facial nerve palsy. Investigations showed leukocytosis and bilateral hilar lymphadenopathy. Which of the following is the most likely diagnosis?
- A. Sarcoidosis (Correct Answer)
- B. Tuberculosis
- C. Lymphoma
- D. Hypersensitive pneumonitis
Explanation: ***Sarcoidosis*** - The combination of **fever**, **night sweats**, **bilateral facial nerve palsy**, **ptosis**, and **bilateral hilar lymphadenopathy** is highly suggestive of **neurosarcoidosis** manifesting as Heerfordt's syndrome (uveoparotid fever) [1]. - **Leukocytosis** is a non-specific finding but can be present due to inflammatory processes in sarcoidosis. *Tuberculosis* - While tuberculosis can cause **fever**, **night sweats**, and **hilar lymphadenopathy** [2] [3], it is less likely to present with **bilateral facial nerve palsy** and **ptosis** simultaneously. - Pulmonary tuberculosis often shows specific patterns like **apical infiltrates** or cavitations, rather than solely bilateral hilar lymphadenopathy, especially without other classic symptoms like productive cough. *Lymphoma* - Lymphoma can cause **fever**, **night sweats**, and **lymphadenopathy** (including hilar) [4]. - However, **bilateral facial nerve palsy** and **ptosis** are not typical primary manifestations of lymphoma and would require other evidence of direct mass effect or widespread infiltration. *Hypersensitive pneumonitis* - This condition is characterized by **inflammation of the lung alveoli** and small airways due to repeated exposure to inhaled antigens, leading to symptoms like cough, dyspnea, and fever. - It typically does **not cause neurological symptoms** such as facial nerve palsy or ptosis, nor is it prominently associated with hilar lymphadenopathy.
Question 5: A patient with a history of chronic liver disease presents with abdominal distension, jaundice, and pruritis. Ascitic fluid analysis revealed a neutrophil count >650 per cubic mm. What is the most likely diagnosis?
- A. Spontaneous bacterial peritonitis (Correct Answer)
- B. Malignant ascites
- C. Tubercular ascites
- D. Intestinal obstruction
Explanation: ***Spontaneous bacterial peritonitis*** - The combination of **chronic liver disease**, **ascites**, and a significantly elevated ascitic fluid **neutrophil count (>250 cells/mm³ is diagnostic)**, in this case, >650 cells/mm³, is highly indicative of spontaneous bacterial peritonitis (SBP). - SBP is a common and serious complication in patients with **cirrhosis** and ascites, characterized by bacterial infection of ascitic fluid without an obvious source. *Malignant ascites* - While malignant ascites can occur in chronic liver disease (e.g., from hepatocellular carcinoma), the ascitic fluid analysis would typically show **cytology positive for malignant cells** and often a **low neutrophil count** unless secondarily infected. - The primary differentiator here is the very high neutrophil count suggesting an acute inflammatory/infectious process. *Tubercular ascites* - Tubercular ascites might present with ascites and abdominal distension, but the ascitic fluid analysis usually shows a **lymphocytic predominance** (high lymphocyte count) rather than a high neutrophil count. - Diagnosis typically involves **adenosine deaminase (ADA) levels**, acid-fast bacilli smear, or culture of ascitic fluid. *Intestinal obstruction* - Intestinal obstruction primarily causes **abdominal pain, distension, nausea, vomiting**, and constipation, with a clinical picture distinct from SBP. - While it can lead to ascites in rare cases (e.g., from bowel ischemia or perforation), the ascitic fluid would not characteristically show such a high neutrophil count unless there was associated perforation and peritonitis.
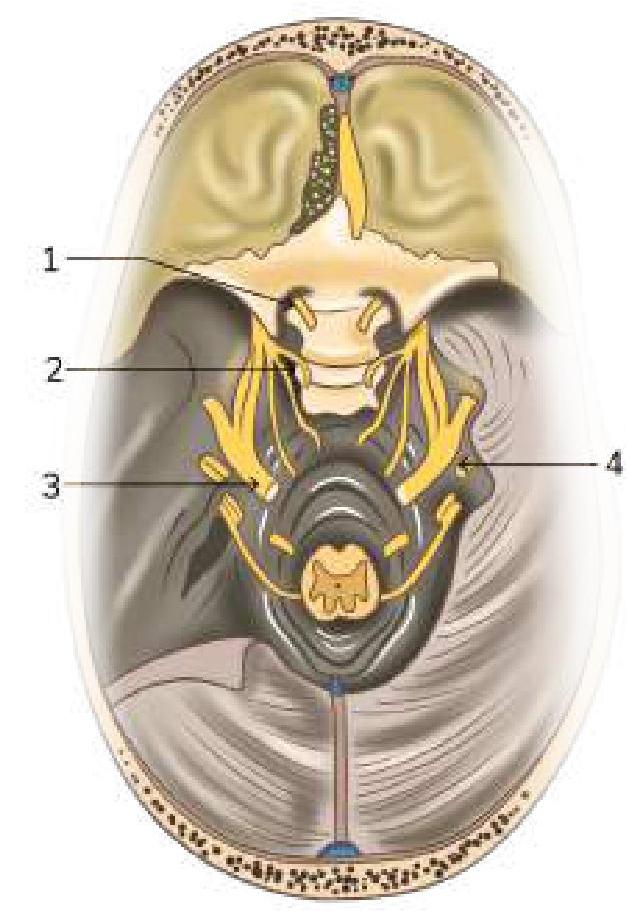
Question 6: A patient presents with a unilateral throbbing headache, photophobia, and excessive lacrimation. He also complains of hemifacial pain on the clenching of teeth. On examination, pupillary reaction, light reflex, and accommodation reflex are normal. Which of the following marked nerves is most likely involved in the above scenario?
- A. Hypoglossal nerve
- B. Oculomotor nerve
- C. Trigeminal nerve (Correct Answer)
- D. Facial nerve
Explanation: ***Trigeminal nerve*** - The patient's symptoms of **unilateral throbbing headache**, **photophobia**, **excessive lacrimation**, and **hemifacial pain exacerbated by clenching teeth** are characteristic of trigeminal autonomic cephalalgias, such as **cluster headache** or **paroxysmal hemicrania**. These conditions involve the trigeminal nerve and its parasympathetic connections. - The image indicates **cranial nerve V** (trigeminal nerve) as structure 2, which has sensory innervation to the face and motor innervation to the muscles of mastication. **Hemifacial pain on clenching teeth** directly implicates the trigeminal nerve. *Oculomotor nerve* - The oculomotor nerve (cranial nerve III) primarily controls most **eye movements** and **pupil constriction**. - While headaches can sometimes affect pupil size (e.g., Horner's syndrome in cluster headache may involve sympathetic fibers that travel with cranial nerves), the core symptoms of facial pain on teeth clenching are not directly related to oculomotor nerve function. The normal pupillary and light reflexes also indicate its intact function. *Hypoglossal nerve* - The hypoglossal nerve (cranial nerve XII) is responsible for **tongue movement**. - Symptoms like headache, facial pain, photophobia, or lacrimation are not associated with hypoglossal nerve dysfunction. *Facial nerve* - The facial nerve (cranial nerve VII) controls **facial expressions**, **taste from the anterior two-thirds of the tongue**, and **lacrimation/salivation**. - While it contributes to lacrimation, the primary symptoms of unilateral throbbing headache and hemifacial pain, particularly exacerbated by teeth clenching, are not characteristic of facial nerve involvement.
Question 7: A patient presents to you with an irregularly irregular pulse of 120/minutes and a pulse deficit of 20. Which of the following would be the jugular venous pressure (JVP) finding?
- A. Normal JVP
- B. Absent a wave (Correct Answer)
- C. Cannon a wave
- D. Raised JVP with normal waveform
Explanation: ***Absent a wave*** - An **irregularly irregular pulse** with a **pulse deficit** strongly suggests **atrial fibrillation (AF)**. - In AF, the atria quiver chaotically instead of contracting effectively, leading to the **absence of a coordinated atrial contraction** and thus an **absent 'a' wave** in the JVP. *Normal JVP* - A normal JVP would show a regular **'a' wave** corresponding to normal atrial contraction. - This is inconsistent with the **irregularly irregular pulse** and **pulse deficit** seen in the patient, which points to a significant atrial arrhythmia. *Cannon a wave* - A **cannon 'a' wave** results from the right atrium contracting against a closed tricuspid valve, leading to a large, prominent wave in the JVP. - This is typically seen in conditions like **complete heart block** or **ventricular tachycardia with AV dissociation**, not atrial fibrillation. *Raised JVP with normal waveform* - A raised JVP with a normal waveform indicates increased right atrial pressure but preserves the normal sequence of atrial contraction and relaxation. - This could be due to conditions like **right heart failure** or **volume overload**, but would still show the presence of an 'a' wave, which is absent in atrial fibrillation.
Question 8: A woman presents to you with fever, arthralgia, ulcers, fatigue for the past six months, and new-onset hematuria. Urine examination reveals RBC casts and proteinuria. What is the likely diagnosis?
- A. Acute interstitial nephritis
- B. Poststreptococcal glomerulonephritis
- C. Lupus nephritis (Correct Answer)
- D. IgA nephropathy
Explanation: ***Lupus nephritis*** - The combination of **fever, arthralgia, oral ulcers, and fatigue** lasting for six months is highly suggestive of **systemic lupus erythematosus (SLE)** [1]. - The new-onset **hematuria, proteinuria, and RBC casts** indicate **glomerulonephritis**, which is a common and serious renal manifestation of SLE, known as lupus nephritis [2]. *Acute interstitial nephritis* - Characterized by acute kidney injury, often following exposure to **medications** (e.g., NSAIDs, antibiotics) or infections. - Typically presents with sterile pyuria, eosinophilia, and white cell casts, not hemorrhagic urine and RBC casts. *Poststreptococcal glomerulonephritis* - Occurs **1-3 weeks after a streptococcal infection** (e.g., pharyngitis, impetigo) and presents with acute nephritic syndrome. - While it causes hematuria and proteinuria, the prolonged systemic symptoms (arthralgia, ulcers, fatigue) and the absence of a recent streptococcal infection make it less likely. *IgA nephropathy* - Often presents with **recurrent episodes of gross hematuria**, usually developing within days of an upper respiratory tract infection. - It does not typically present with the broad array of systemic symptoms like chronic fever, arthralgia, and oral ulcers seen in this patient.
Question 9: A male patient diagnosed with tuberculosis took complete treatment. Sputum examination was done after the completion of the intensive and the continuation phases. It was found to be negative. What is the status of the patient?
- A. Cured (Correct Answer)
- B. Treatment completed
- C. Lost to follow up
- D. Treatment failed
Explanation: ***Cured*** - A patient is declared **cured** if they have completed the full course of treatment and have achieved **two negative sputum smear results**, with one at the end of the intensive phase and another at the completion of the treatment [1]. - This indicates that the **infection has been eradicated**, and the patient is no longer infectious. *Treatment completed* - This status applies when a patient has **completed the full treatment course** but does not have documented sputum smear results that meet the criteria for "cured." - While treatment was completed, the **bacteriological status is not confirmed** in the same way as for a cured patient. *Lost to follow up* - This term describes a patient who was **enrolled in treatment but was interrupted** for a specific period (e.g., two consecutive months or more) and their outcome cannot be determined. - They **ceased to attend follow-up appointments** and their treatment completion or success is unknown. *Treatment failed* - This status is assigned when a patient remains **sputum smear-positive at the end of the intensive phase** or at the end of the treatment, or if they initially converted to negative but later became positive again [1]. - It signifies that the **treatment regimen was ineffective** in eradicating the infection.
Question 10: A woman with recurrent diarrhea is prescribed a broad-spectrum antibiotic. Which of the following statements is not true regarding Clostridium difficile infection?
- A. Pseudomembrane is a layer of inflammatory debris
- B. Oral fidaxomicin is used for treatment
- C. It is toxin mediated
- D. IgM assay is used to confirm the diagnosis of Clostridium difficile infection. (Correct Answer)
Explanation: ***IgM assay is used to confirm the diagnosis of Clostridium difficile infection*** - An **IgM assay** is **not** the standard or recommended method for diagnosing *Clostridium difficile* infection (CDI). - Diagnosis typically relies on detecting **toxins (A and B)** in stool samples through antigen-based tests, PCR, or enzyme immunoassays [1]. *Oral fidaxomicin is used for treatment* - **Fidaxomicin** is an **oral macrolide antibiotic** specifically approved and highly effective for treating *C. difficile* infection, especially recurrent cases. - It works by inhibiting bacterial RNA polymerase, leading to bactericidal activity against *C. difficile* with minimal systemic absorption. *It is toxin mediated* - The pathogenicity of *C. difficile* is primarily mediated by its **exotoxins, Toxin A (enterotoxin)** and **Toxin B (cytotoxin)** [1]. - These toxins cause mucosal inflammation, increased permeability, and cell death in the colon, leading to the characteristic symptoms of CDI. *Pseudomembrane is a layer of inflammatory debris* - **Pseudomembranes** are a hallmark pathological feature of severe *C. difficile* colitis, visible during colonoscopy [1]. - They consist of an inflammatory exudate composed of **necrotic epithelial cells, fibrin, neutrophils, and mucus**, forming raised yellow-white plaques on the colonic mucosa.